Downloaded 20 times

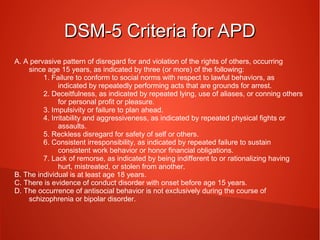
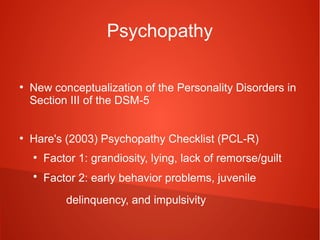

This document discusses Antisocial Personality Disorder (APD) by outlining the DSM-5 criteria, comparing it to psychopathy, examining risk factors and heritability, the development from conduct disorder to APD, and treatment options. The key points are: the DSM-5 criteria for APD includes a disregard for others' rights since age 15; psychopathy is assessed using Hare's Psychopathy Checklist measuring grandiosity and impulsivity; risk factors include biological and environmental influences like abuse or unstable parenting; those with childhood-onset conduct disorder are more likely to develop APD; and treatment focuses on reducing substance abuse and using mentalization-based therapy.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


