This document provides an overview of white blood cell pathology, including classifications of leukocytosis, leukopenia, leukemia, and leukemoid reactions. It discusses:
1. Leukocytosis is classified based on cause (physiological vs pathological), pathogenesis (reactive, redistributive, tumorous), and cell type (neutrophilic, eosinophilic, etc.). Leukopenia is also classified based on origin, cell type affected, and pathogenesis.
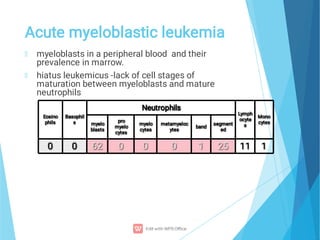
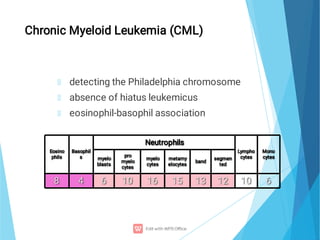
2. Leukemias are classified as acute or chronic, myeloid or lymphatic. Acute leukemias are characterized by an inability of cells to differentiate and a "leukemic gap" in maturation. Chronic leukemias








































































![White blood cells [wbc]](https://cdn.slidesharecdn.com/ss_thumbnails/whitebloodcellswbc-180530054405-thumbnail.jpg?width=640&height=640&fit=bounds)










































