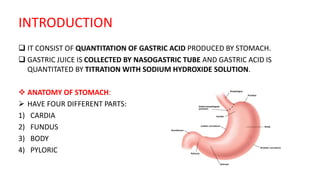
This document provides an overview of gastric analysis, which quantifies gastric acid production by the stomach. It discusses the anatomy and physiology of the stomach and acid secretion. Methods for collecting gastric juice samples via nasogastric tube are described, including basal acid output measurement and stimulation with pentagastrin to measure peak acid output. Normal ranges for acidity measurements and their indications are provided. The document outlines contraindications and alternative tests like Hollander's test and fractional test meal.