Download as PDF, PPTX


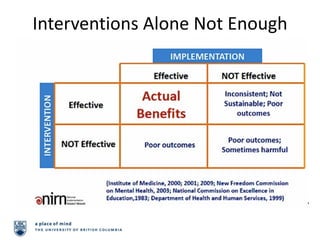


The document discusses implementation science, focusing on the effective and sustainable integration of evidence-based interventions to reduce injuries in organizations. It identifies key barriers such as the lack of adoption, fidelity, sustainability, and scalability of interventions. Furthermore, it emphasizes the importance of aligning interventions with organizational practices, ensuring adequate resources, and fostering readiness among implementers and stakeholders.






































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)
















