Downloaded 10 times

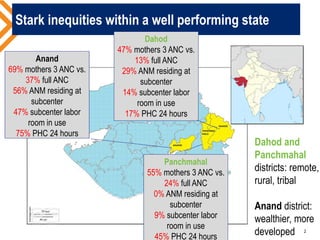






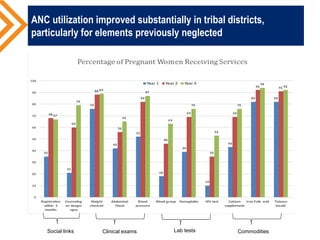
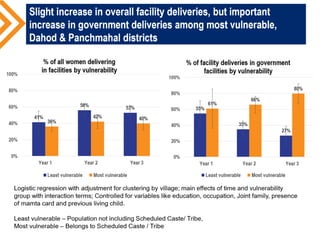
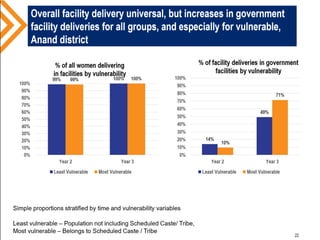

The document discusses a case study from Gujarat, India, focusing on community action for maternal health in rural areas and the disparities in service utilization across different districts. It highlights key strategies used by NGOs to improve accountability and service delivery for maternal health, leading to increased antenatal care (ANC) utilization and improved health outcomes. The findings emphasize the critical role of community participation and NGO involvement in enhancing both demand and supply-side barriers in healthcare services.






















































































