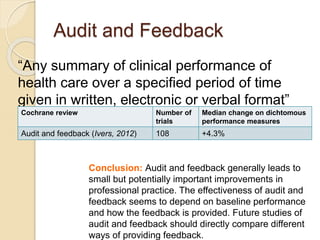
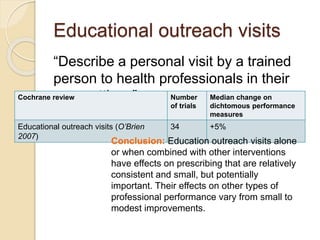
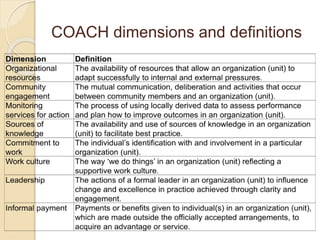
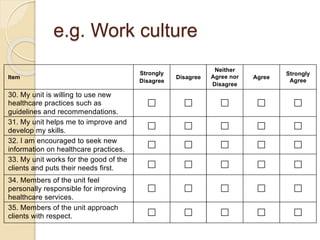
This document discusses implementation strategies for improving healthcare practices. It defines implementation strategies as methods used to promote the adoption of clinical programs. Effective strategies include assessing current performance, analyzing barriers and facilitators, developing an implementation plan, and continuous evaluation. Common strategies discussed include audit and feedback, educational outreach, reminders, and financial incentives. The document notes that no single strategy is clearly most effective and that tailoring strategies to the local context is important. It also introduces several tools for assessing the context, such as the COACH framework which examines multiple dimensions like work culture, leadership, and resources.