
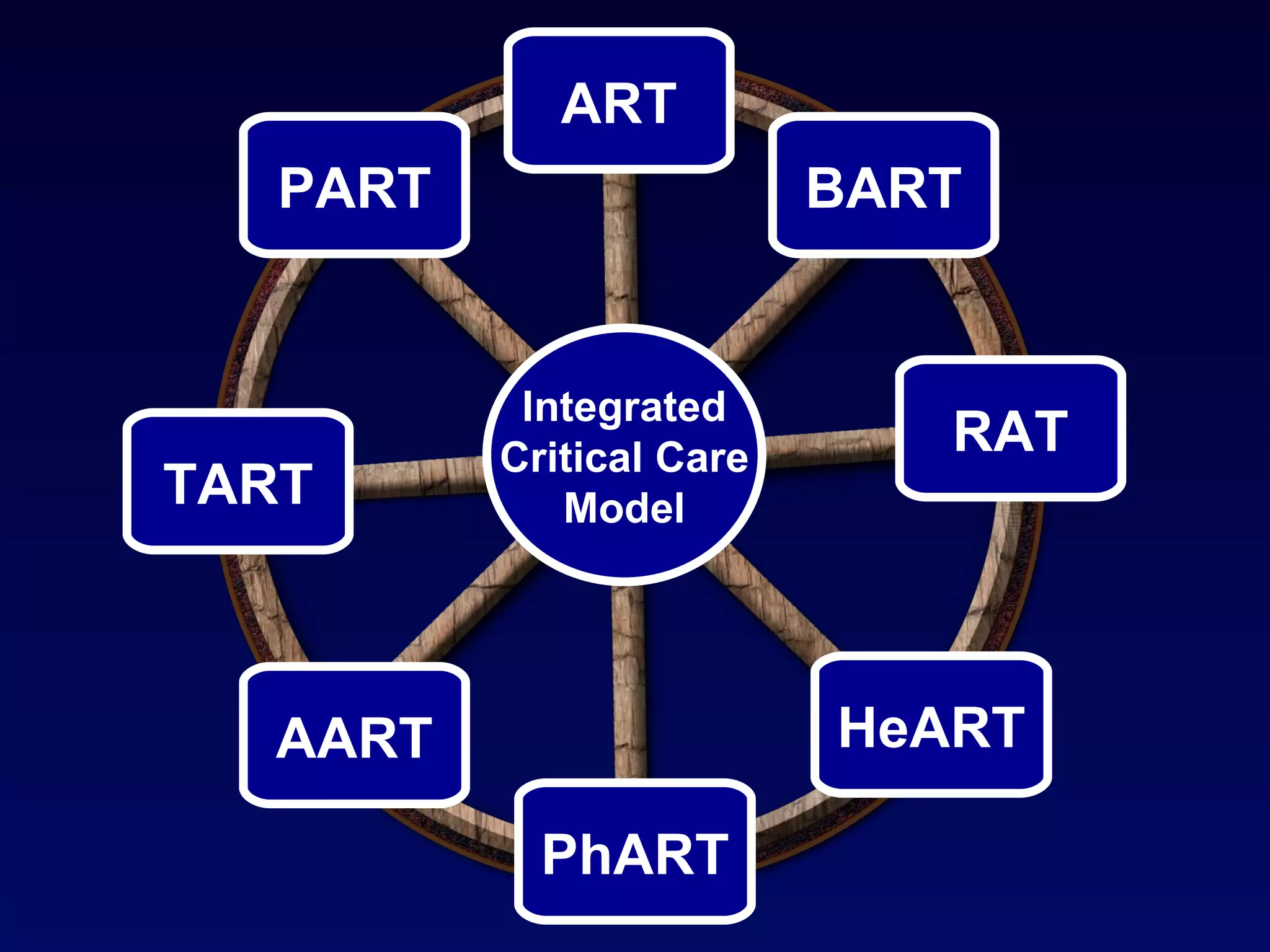
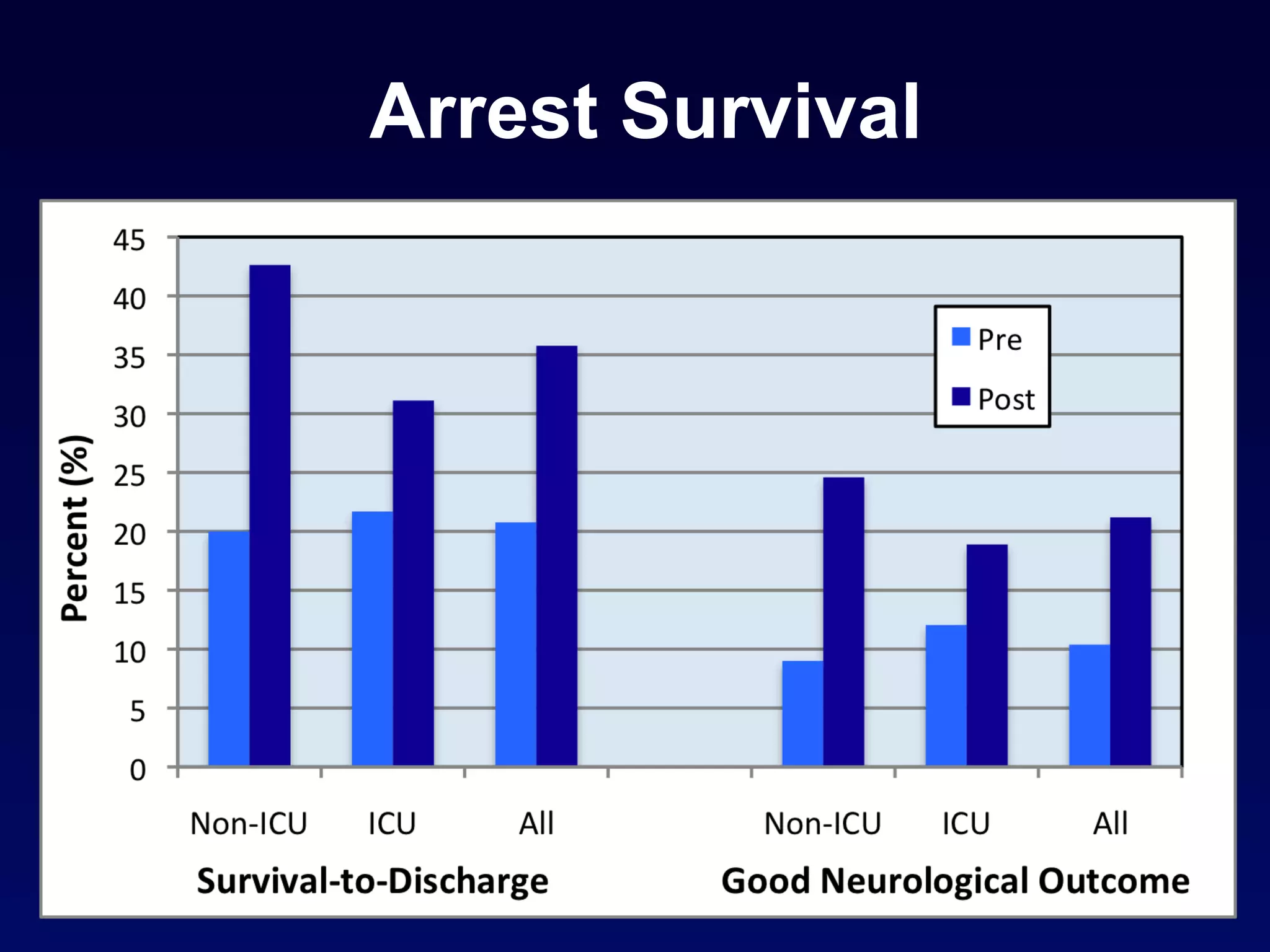







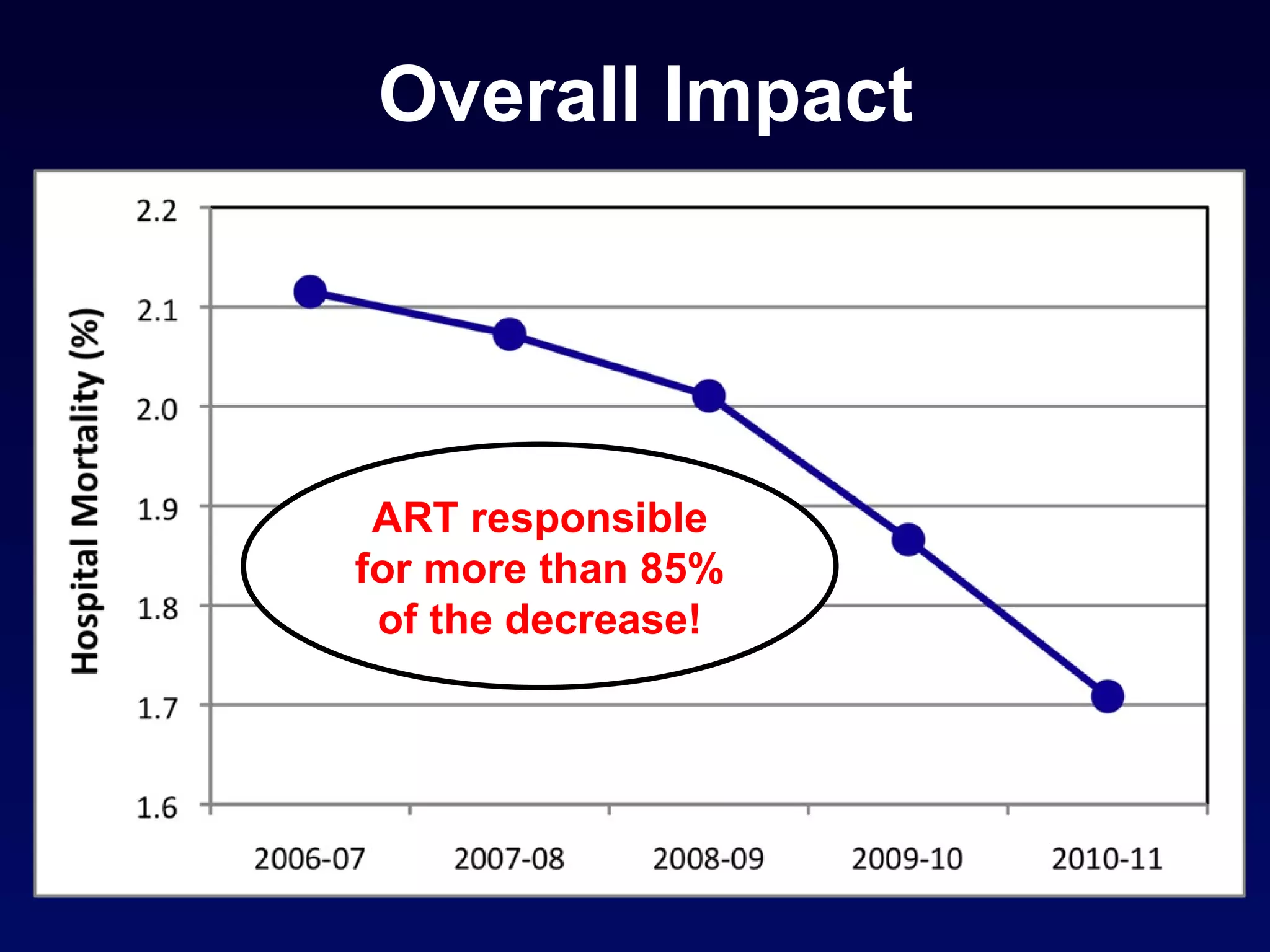
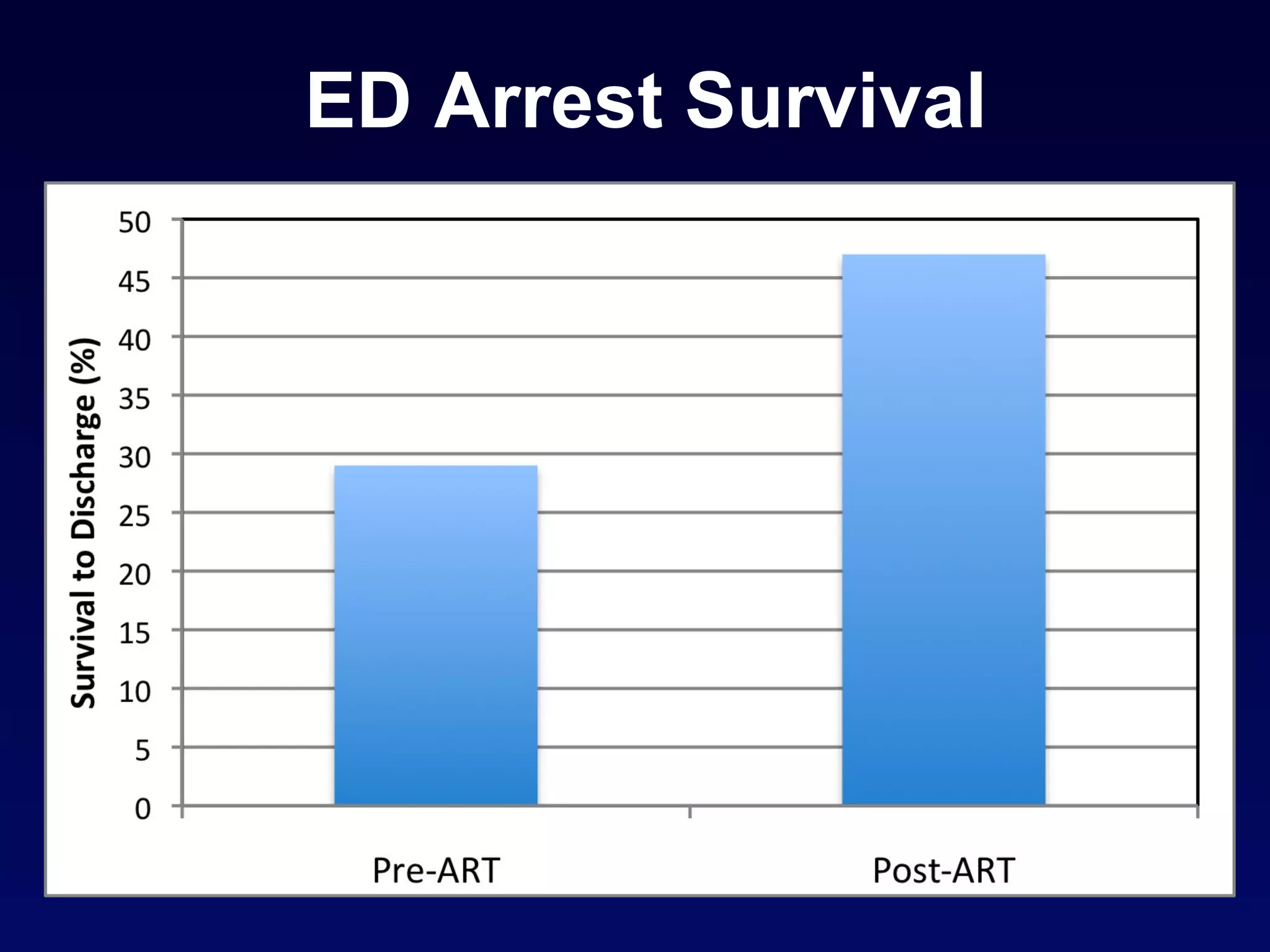













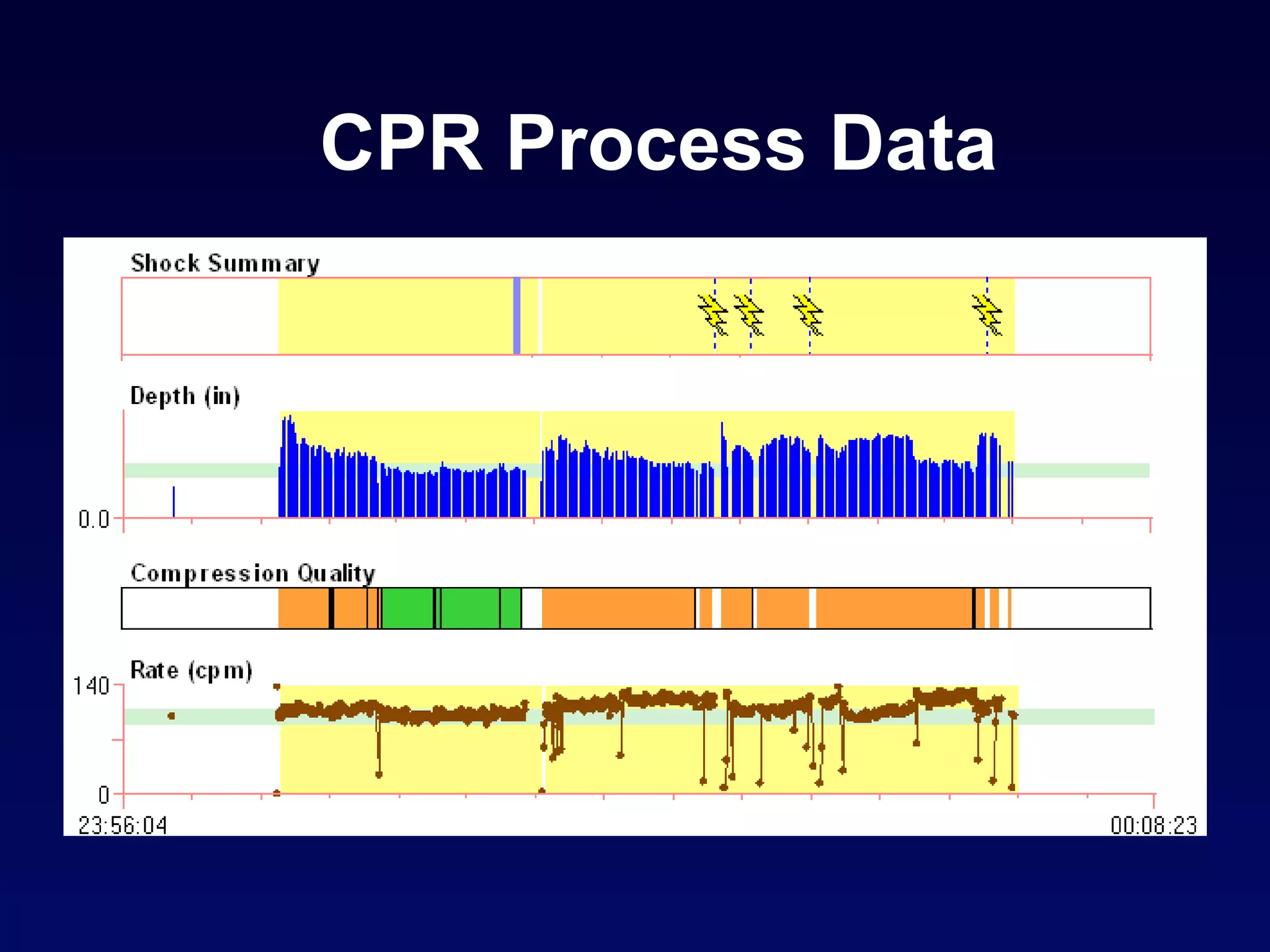

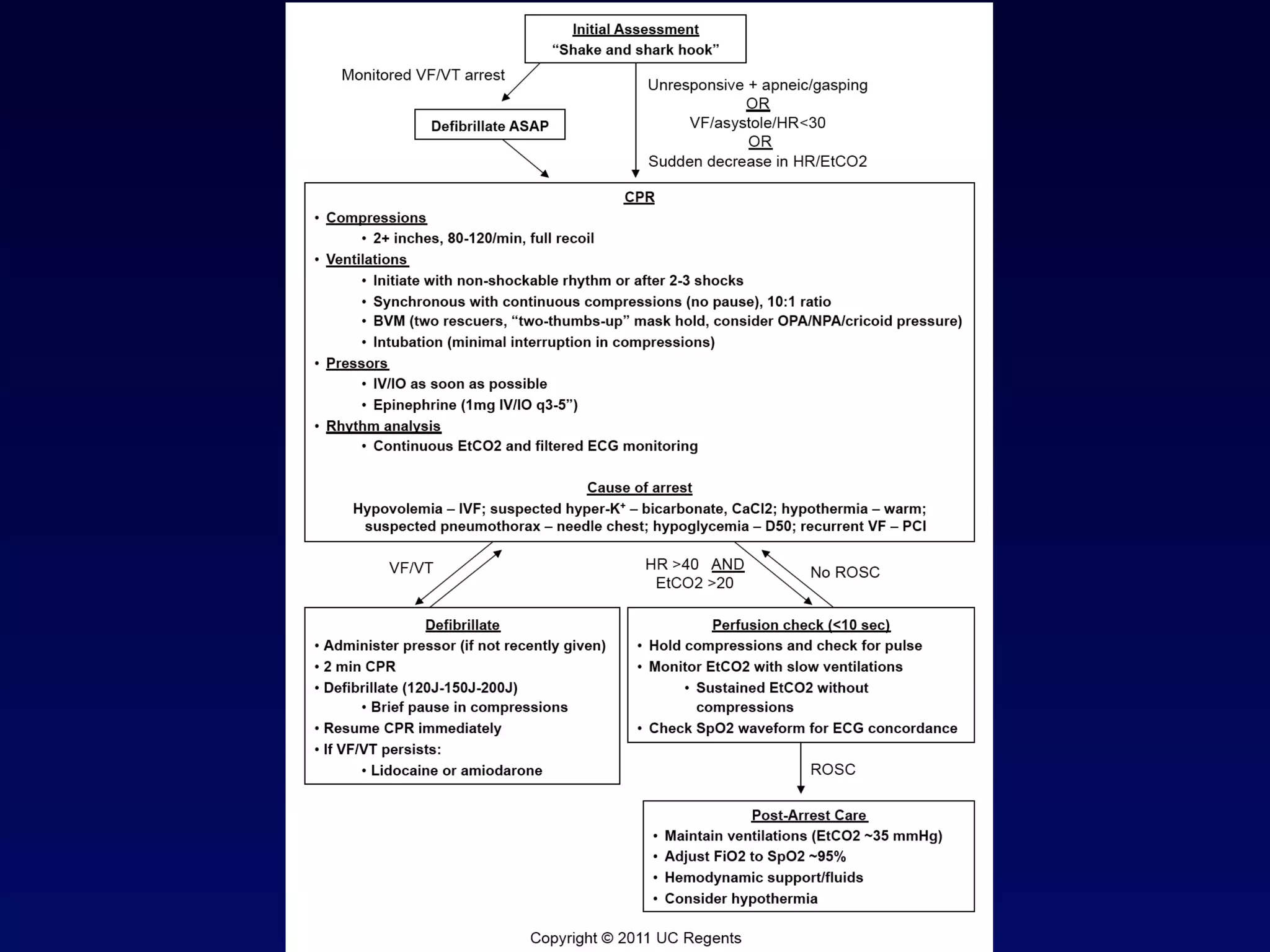
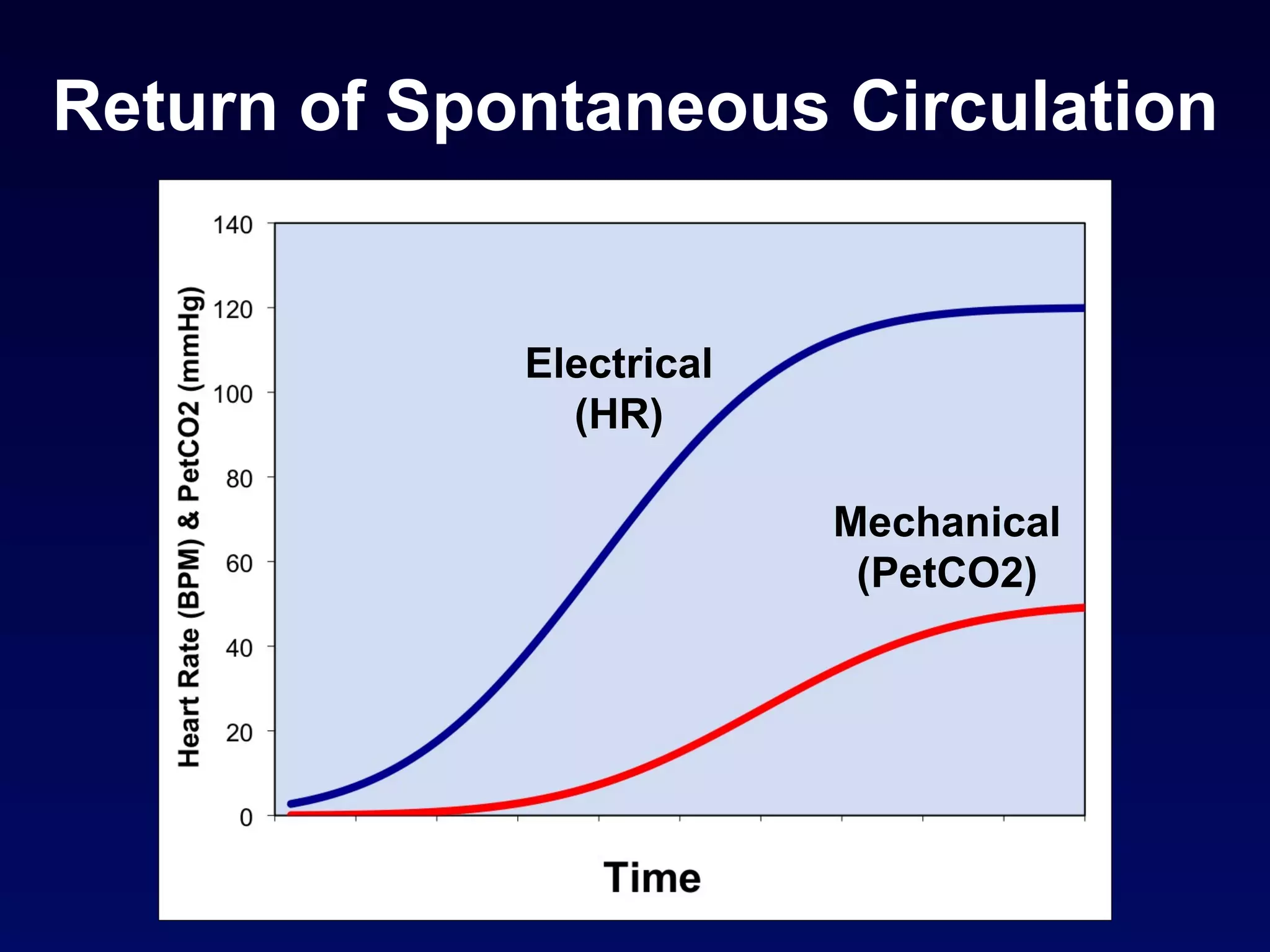


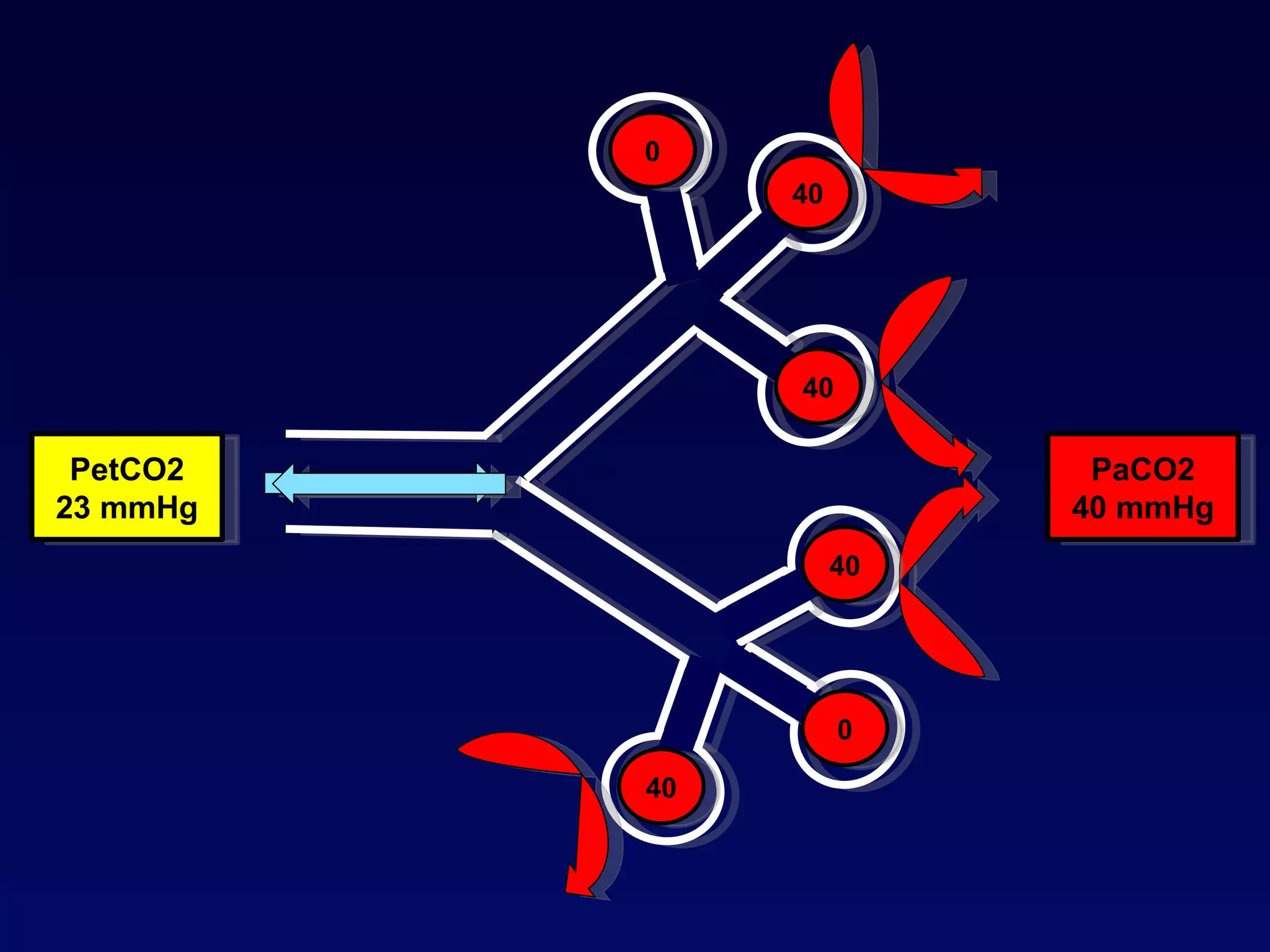

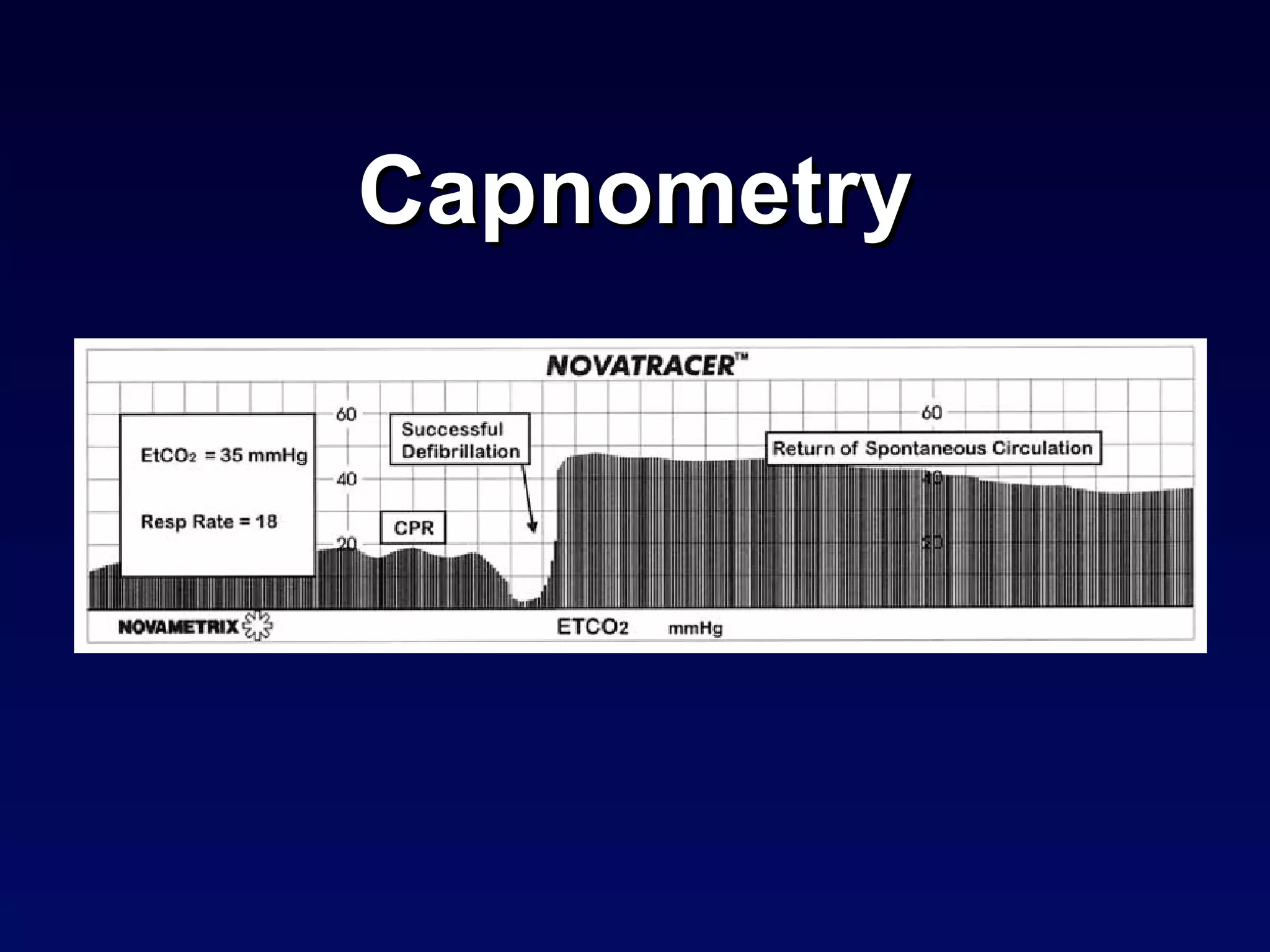






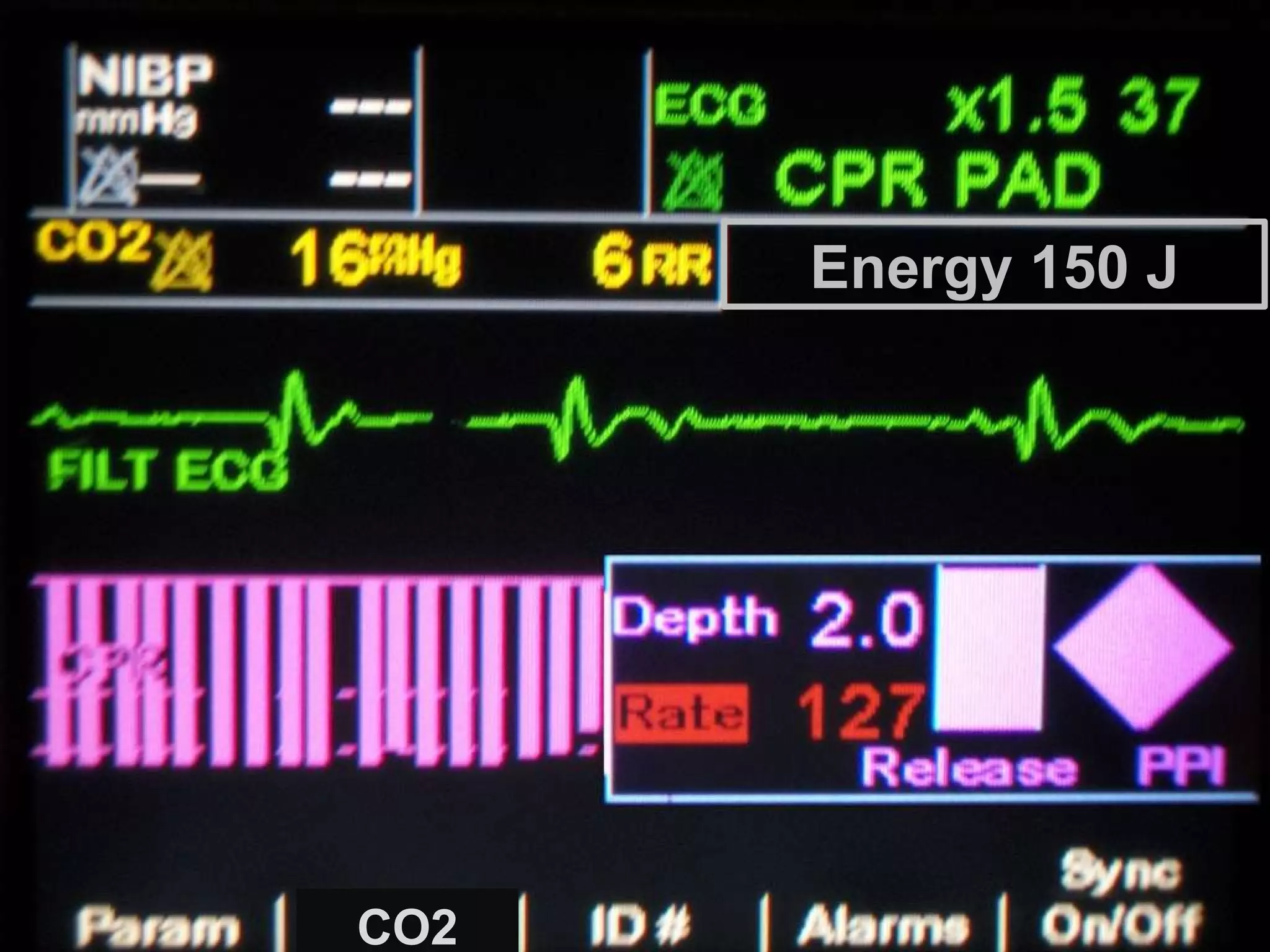
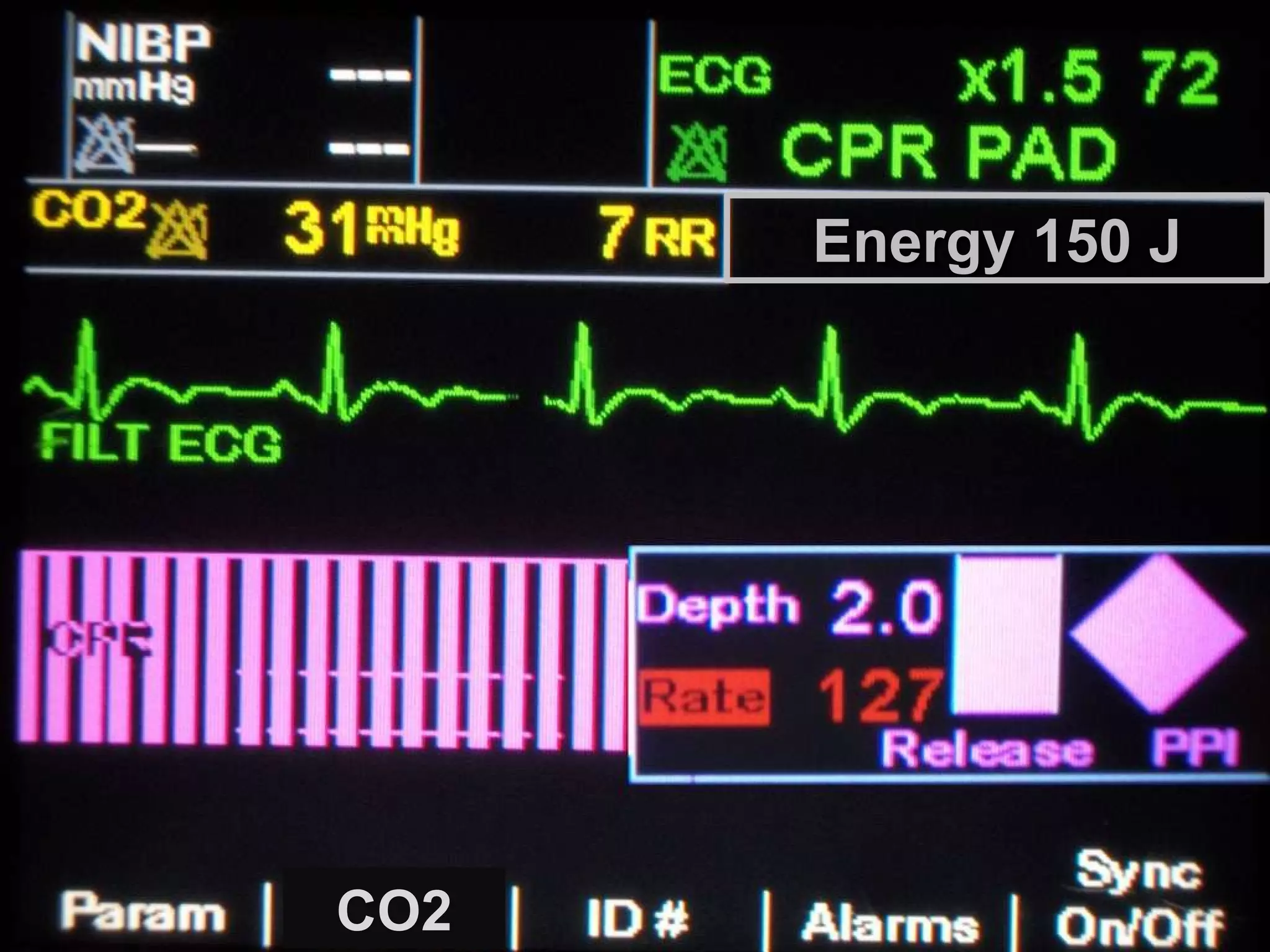

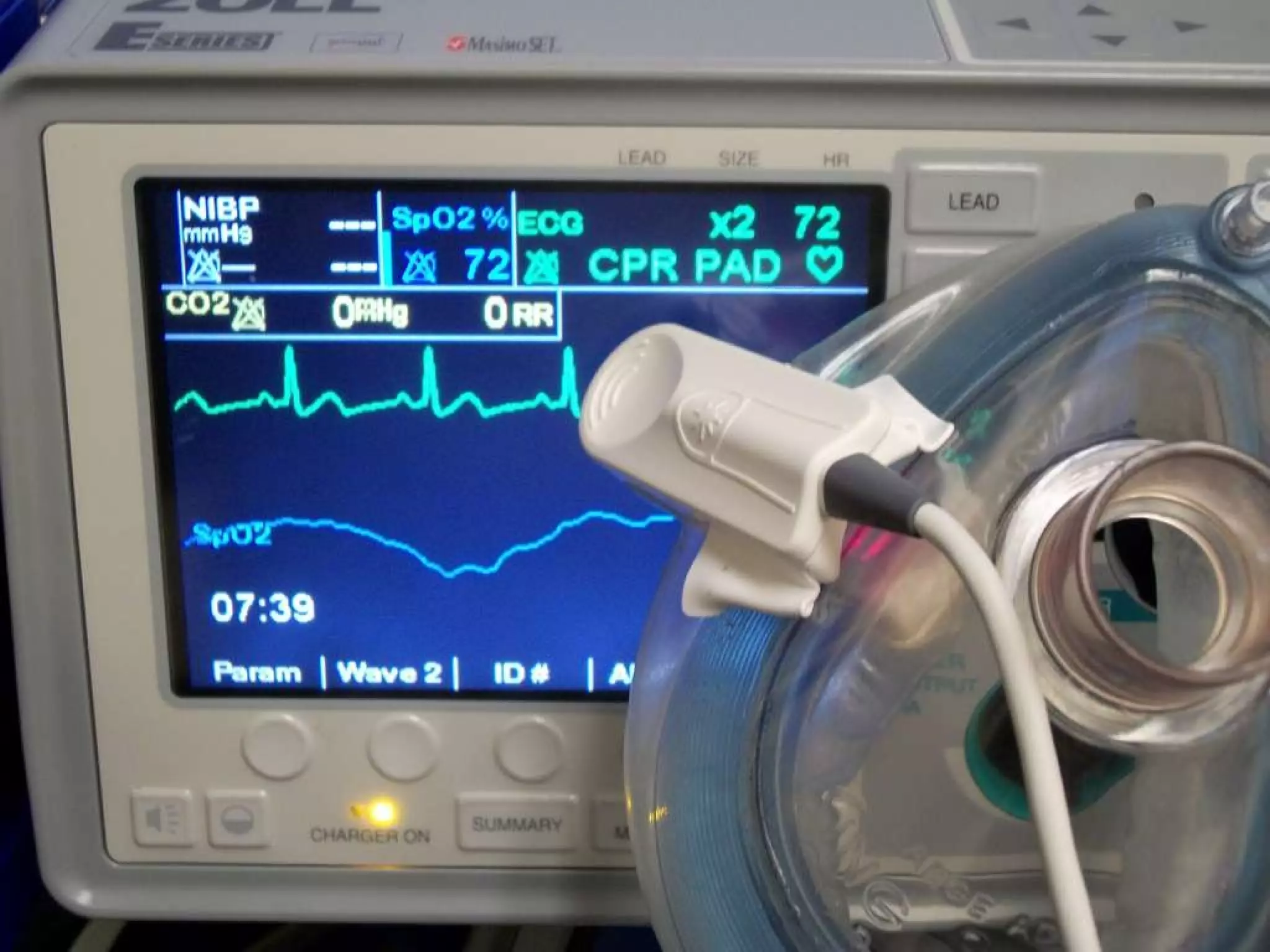
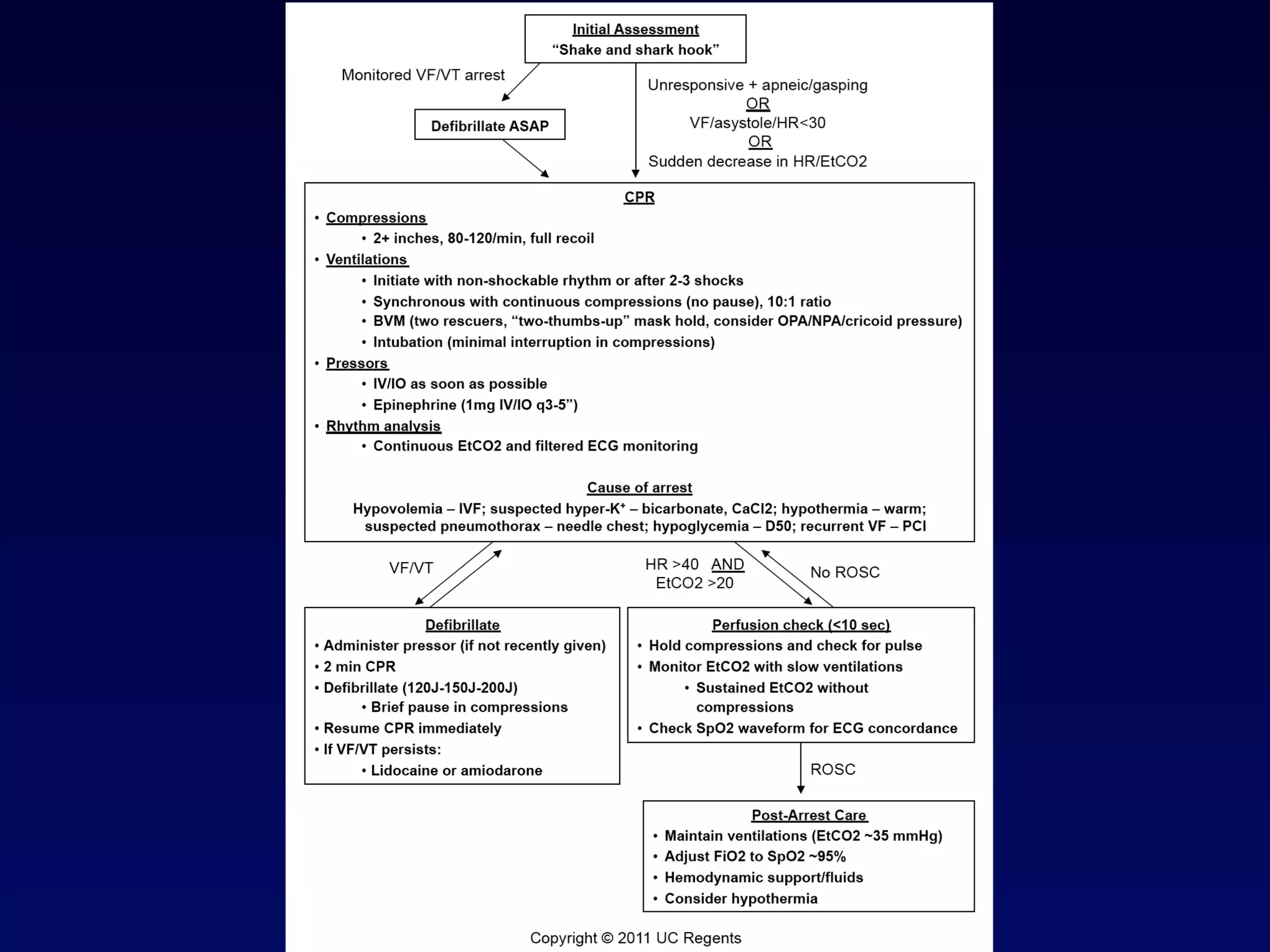


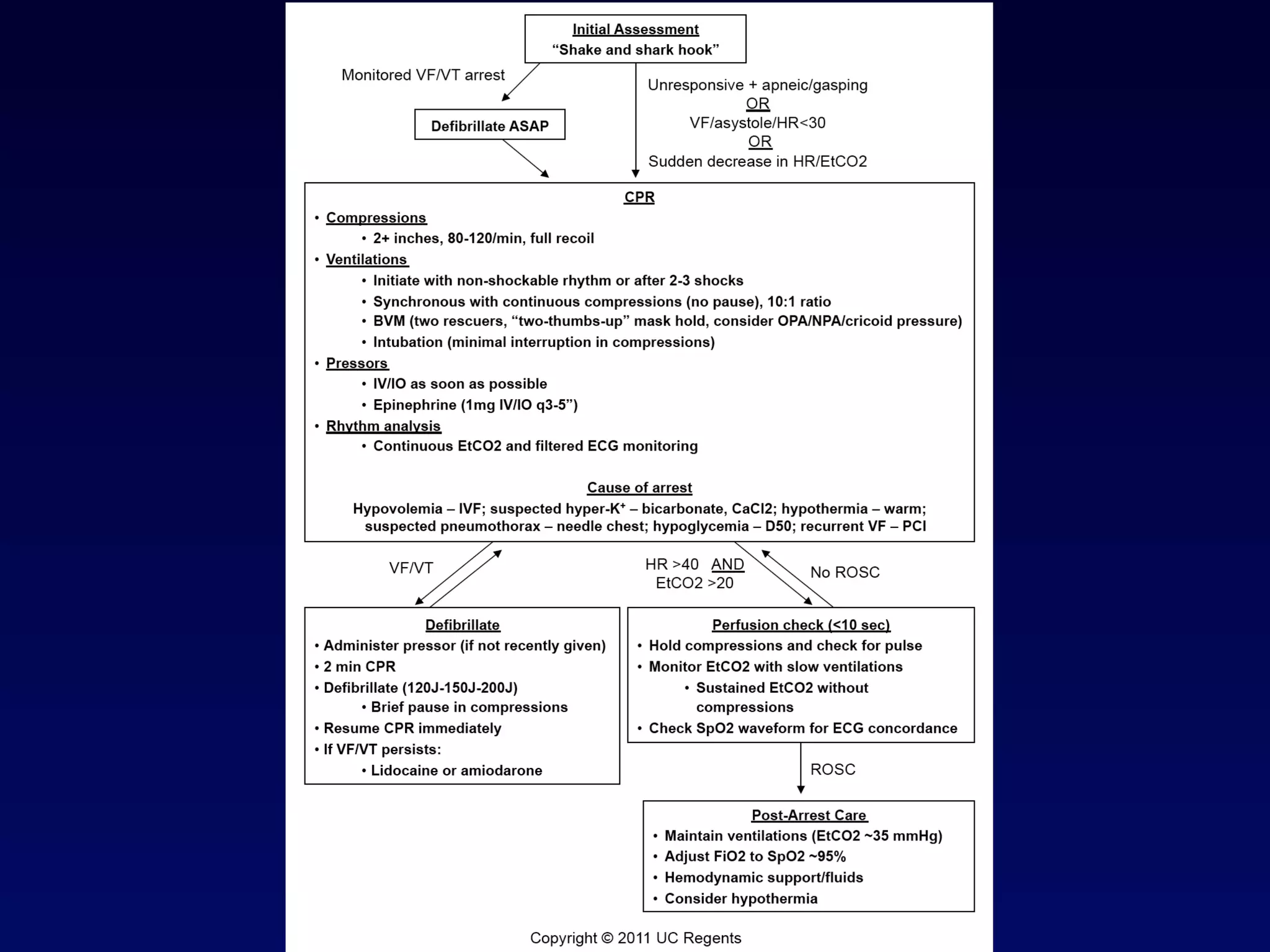


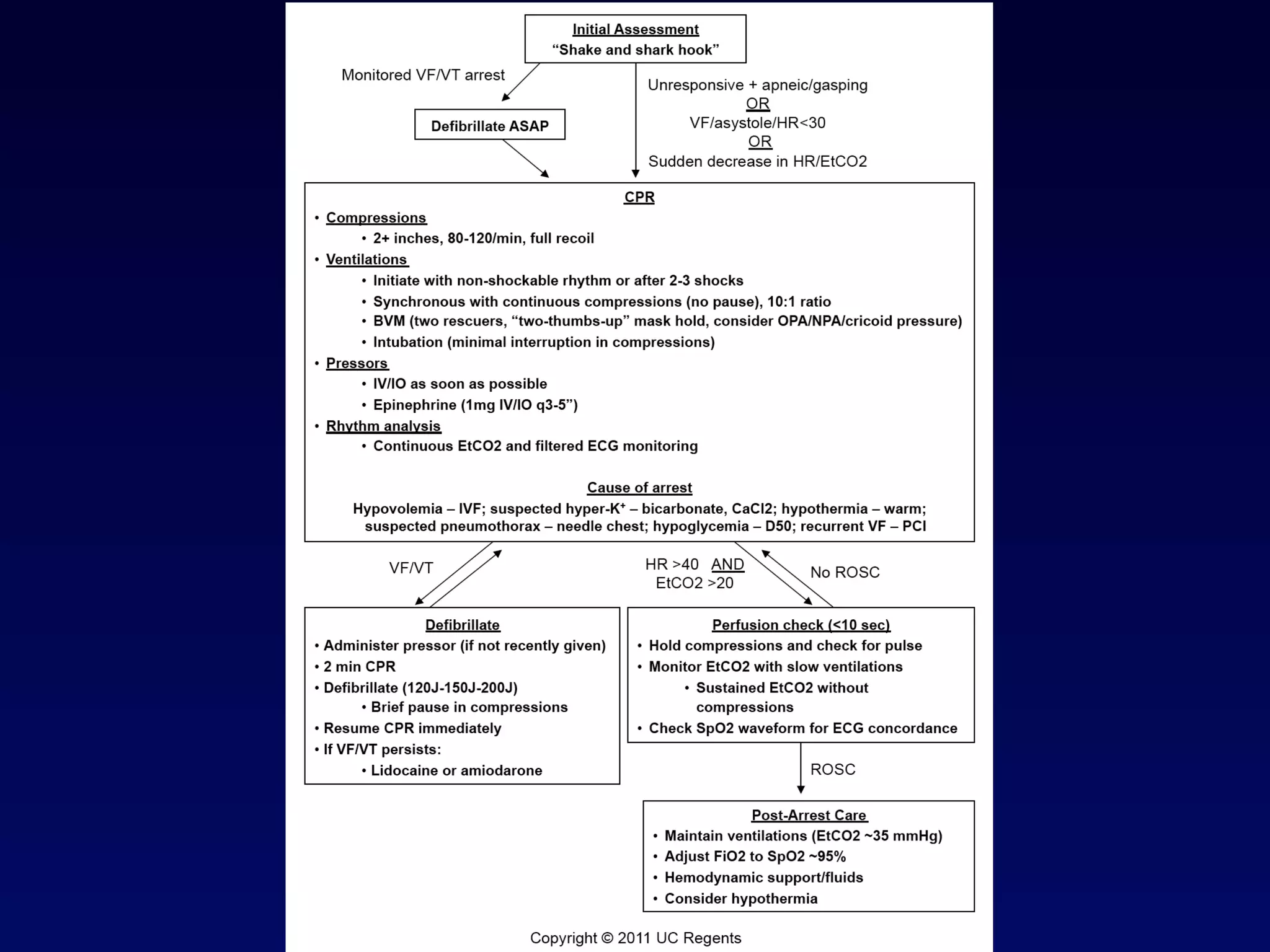




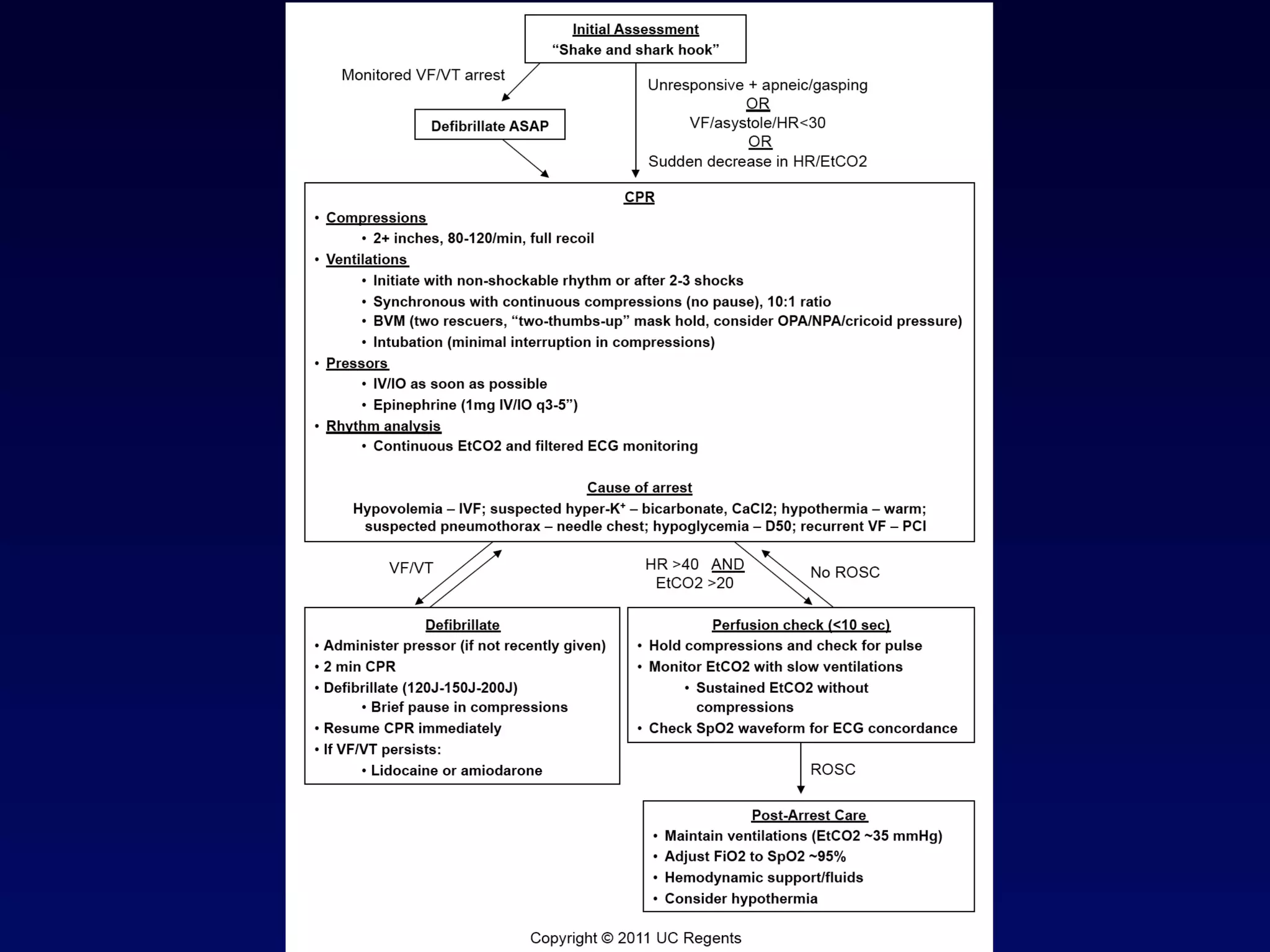













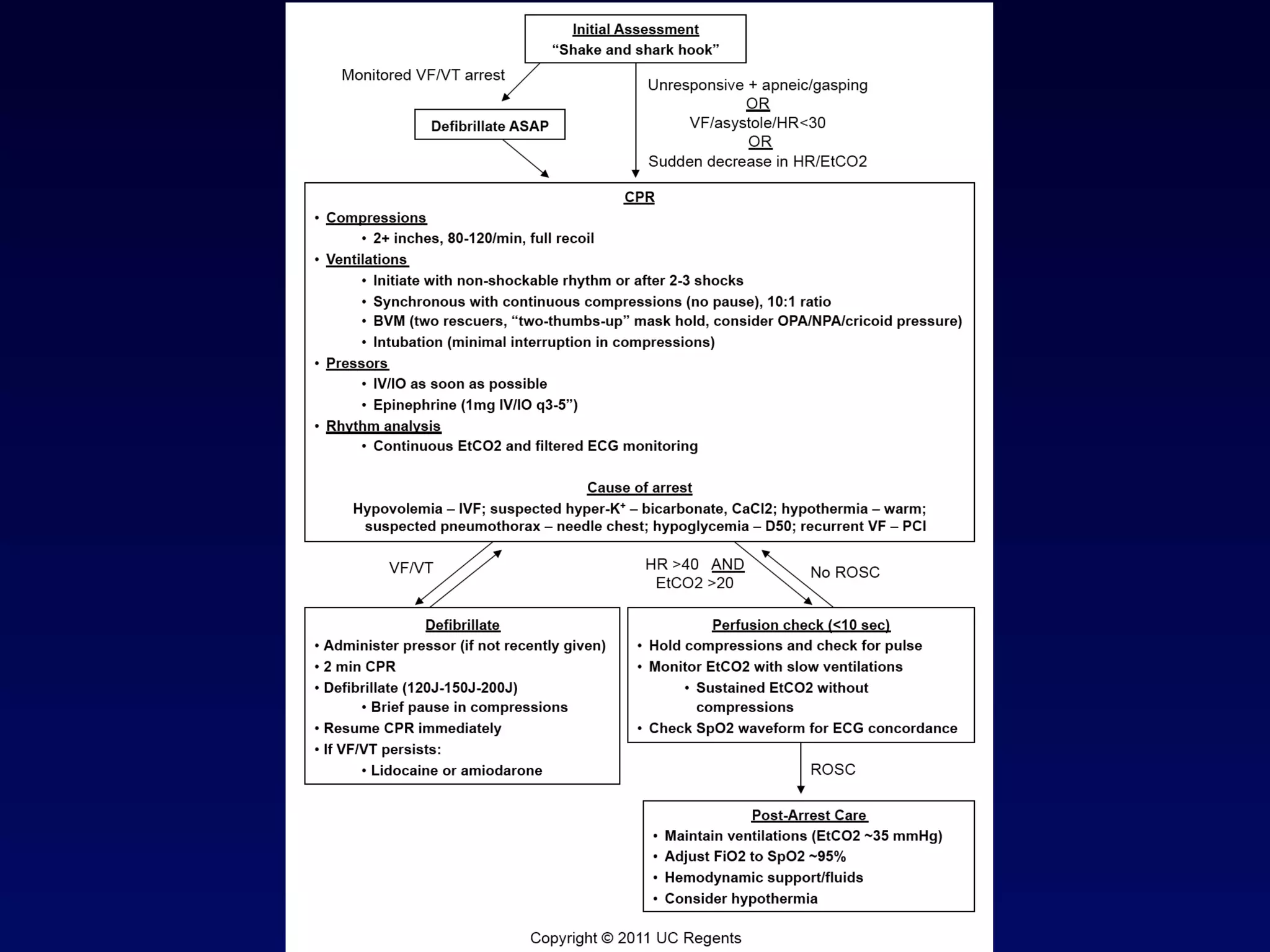























The document outlines the Advanced Resuscitation Techniques (ART) model for improving resuscitation outcomes. It describes seven commandments of cardiac arrest care, including high-quality chest compressions, use of pressors, ventilation techniques, and a focus on prevention. Sample patient cases and data on outcomes with the ART model in San Diego show increased survival rates from cardiac arrest.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












