Downloaded 664 times







![Universal Definition of Myocardial Infarction
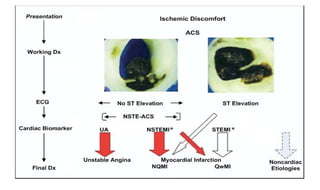
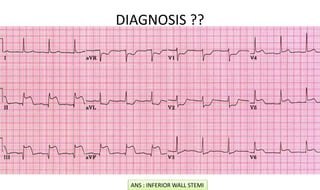
• The term acute myocardial infarction (MI) should be used when there is evidence of
myocardial necrosis in a clinical setting consistent with acute myocardial ischemia.
Under these conditions, any one of the following criteria meets the diagnosis for MI
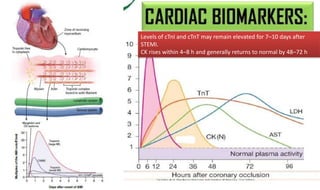
• Detection of a rise and/or fall of cardiac biomarker values (preferably cardiac troponin
[cTn]) with at least one value above the 99th percentile upper reference limit (URL)
and with at least one of the following:
• • Symptoms of ischemia
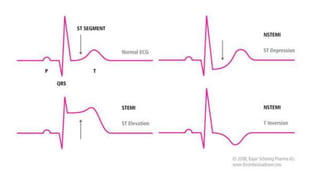
• • New or presumed new significant ST-segment T-wave (ST-T) changes or new left
bundle branch block (LBBB)
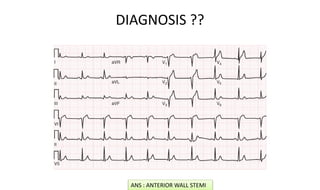
• • Development of pathologic Q waves in the electrocardiogram (ECG)
• • Imaging evidence of new loss of viable myocardium or new regional wall motion
abnormality
• • Identification of an intracoronary thrombus by angiography or autopsy](https://image.slidesharecdn.com/adultblsacls2015-180527101656/85/Adult-BLS-ACLS-2015-62-320.jpg)





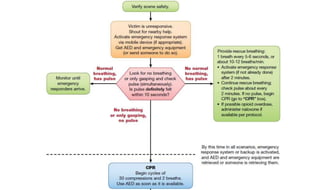
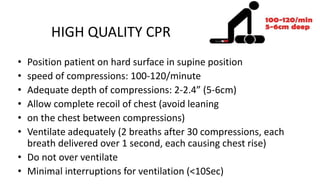
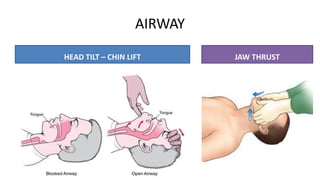
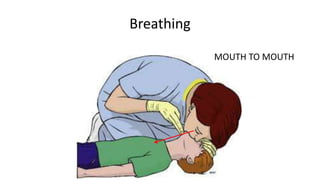
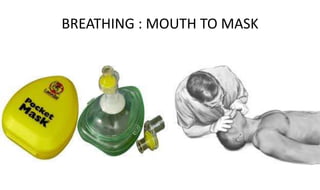
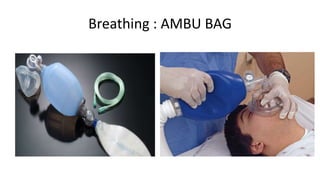
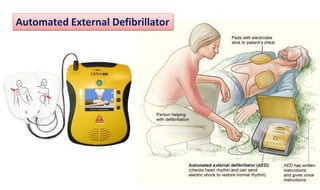
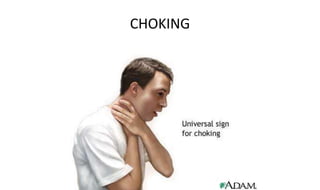
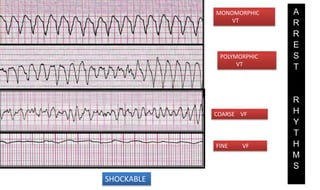
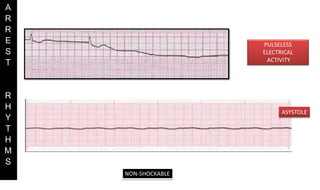
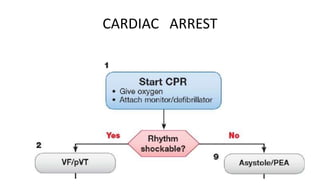
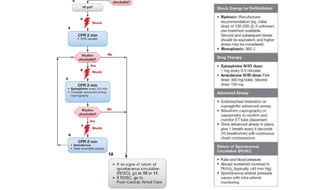
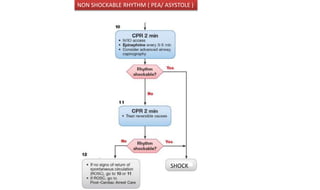
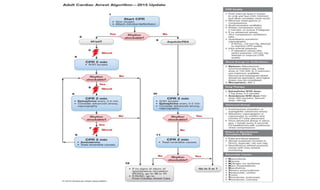
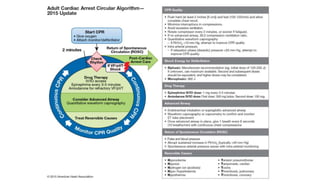
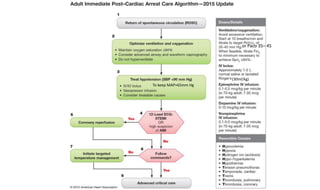
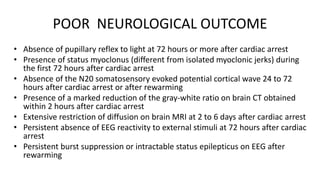
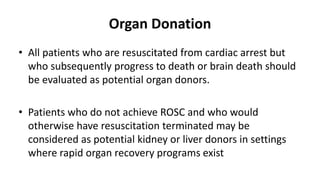
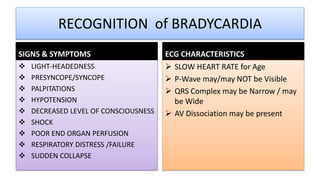
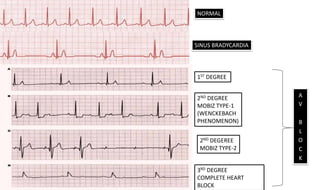
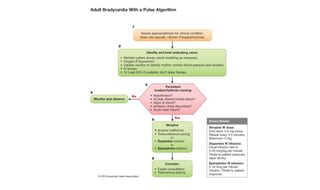
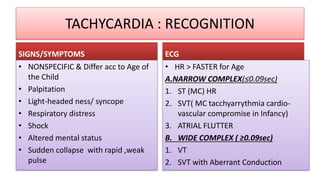
This document provides guidelines for adult BLS and ACLS. It discusses CPR techniques including compressions at a rate of 100-120 per minute with a depth of 2-4 inches. It also discusses airway management, use of an AED, and monitoring during CPR. The document then summarizes algorithms for pulseless arrest, bradycardia, tachycardia, and acute coronary syndrome. It provides details on the management of different cardiac rhythms and guidelines for prognostication, organ donation, and targeted temperature management after cardiac arrest.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












