Downloaded 80 times





















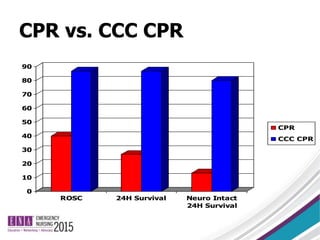
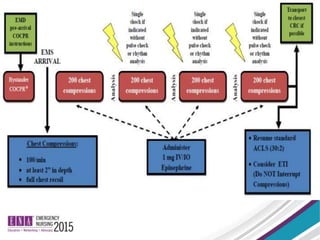





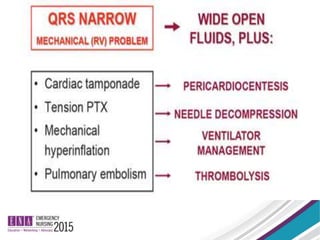
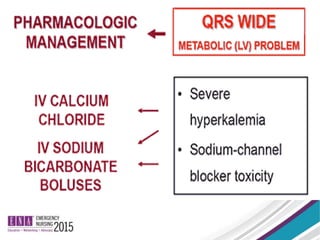






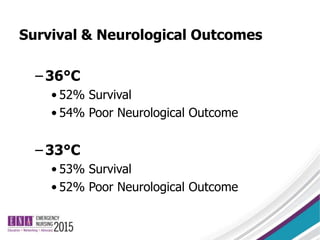




The document discusses advancements in managing adult cardiac arrest beyond standard ACLS protocols, emphasizing high-quality CPR, continuous chest compressions, and alternative drugs for treatment. It critiques the efficacy of epinephrine and introduces hemodynamic directed dosing as a potentially superior approach. Furthermore, it highlights the importance of targeted temperature management post-resuscitation for improved outcomes.























































































