Downloaded 274 times







![Contraindications and exclusion
criteria for TAVI are as follows:
Evidence of an acute MI at 1 month or less
before the intended treatment (defined as Q-wave
MI, or non–Q-wave MI with CK-MB twice normal in
the presence of MB elevation and/or troponin level
elevation [WHO definition].](https://image.slidesharecdn.com/tavi-161220092345/75/Tavi-Transcatheter-Aortic-Valve-Replacement-TAVI-TAVR-13-2048.jpg)







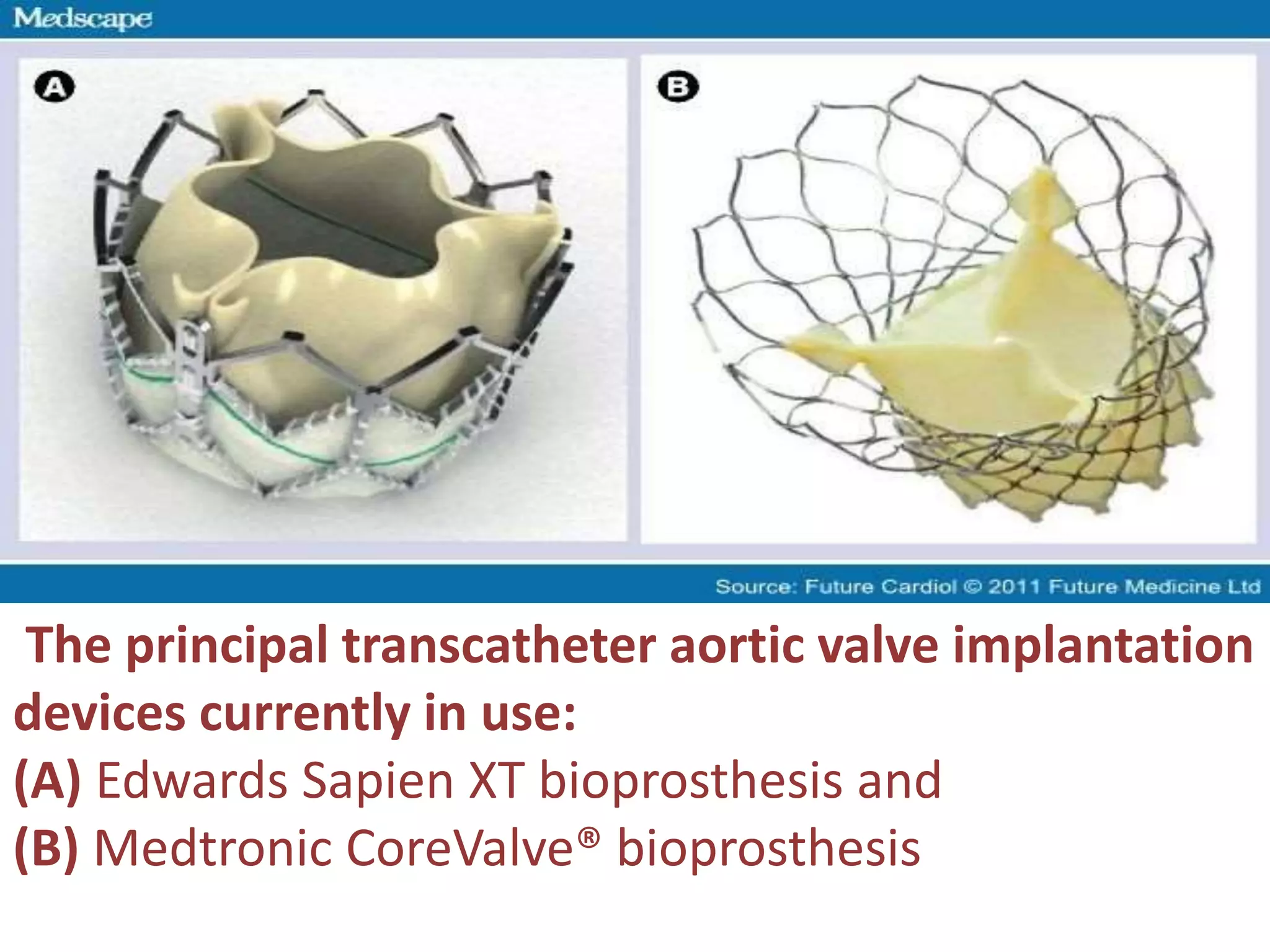






Transcatheter aortic valve implantation (TAVI) has been developed as an alternative to surgical aortic valve replacement for high-risk patients. TAVI involves threading a collapsible valve through blood vessels and implanting it to replace the diseased valve. Over 30,000 high-risk patients with severe aortic stenosis have undergone TAVI, based on evidence from studies showing it is safer than surgery for this group. TAVI indications may expand as longer-term data on outcomes becomes available and the procedure requires a multidisciplinary team approach and dedicated training.






















































































