CONTENTS
Introduction
Definition–flap
Full mucoperiosteal flap
Partial thickness flap
What is the need for various flap
designs?
Classification
Semilunar flap
Trapezoidal flap
Envelope flap
Triangular flap
Rectangular flap
Oschenbein –lubeke flap
Papilla base flap
Palatal flaps
Palatal flap by wustrow
Palatal flap by wassmund
Palatal flap by wilger and partsch
Palatal flap by fisher
Flap reflection
Flap retraction
Time of retraction
Healing
Review of literature
Conclusion
References
3.
INTRODUCTION
Establishing goodsurgical access requires considerable
pre-surgical planning ,and involves numerous anatomic
and physiologic considerations
The endodontic surgeon should understand the total
concept of proper surgical access, and develop a
systematic approach to pre-surgical planning for each
peri-radicular surgery case.
4.
There are twomajor components of surgical access
Visual access
enables the
endodontist to view
the entire surgical
field.
Manipulative access
helps the surgeon to
carry all the
surgical steps
without hindrance
Castellucci A. Access cavity and endodontic anatomy. Endodontics. 2004;1:245-329.
5.
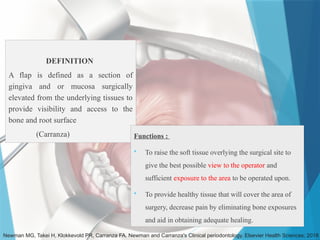
DEFINITION
A flap isdefined as a section of
gingiva and or mucosa surgically
elevated from the underlying tissues to
provide visibility and access to the
bone and root surface
(Carranza)
Newman MG, Takei H, Klokkevold PR, Carranza FA. Newman and Carranza's Clinical periodontology. Elsevier Health Sciences; 2018
Functions :
To raise the soft tissue overlying the surgical site to
give the best possible view to the operator and
sufficient exposure to the area to be operated upon.
To provide healthy tissue that will cover the area of
surgery, decrease pain by eliminating bone exposures
and aid in obtaining adequate healing.
6.
What is theneed for various flap designs?
Numerous variations occur both anatomically and
physiologically in the oral cavity.
These variations should be considered in the pre surgical
planning to achieve good surgical access.
Various complicating factors like dehiscence, gingival
recession and other complicating factors must be
anticipated and incorporated into the pre surgical
planning.
Castellucci A. Access cavity and endodontic anatomy. Endodontics. 2004;1:245-329.
7.
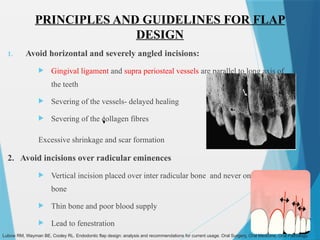
PRINCIPLES AND GUIDELINESFOR FLAP
DESIGN
1. Avoid horizontal and severely angled incisions:
Gingival ligament and supra periosteal vessels are parallel to long axis of
the teeth
Severing of the vessels- delayed healing
Severing of the collagen fibres
Excessive shrinkage and scar formation
2. Avoid incisions over radicular eminences
Vertical incision placed over inter radicular bone and never on radicular
bone
Thin bone and poor blood supply
Lead to fenestration
Lubow RM, Wayman BE, Cooley RL. Endodontic flap design: analysis and recommendations for current usage. Oral Surgery, Oral Medicine, Oral Pathology.
8.
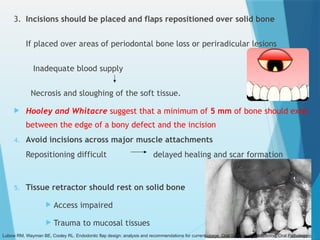
3. Incisions shouldbe placed and flaps repositioned over solid bone
If placed over areas of periodontal bone loss or periradicular lesions
Inadequate blood supply
Necrosis and sloughing of the soft tissue.
Hooley and Whitacre suggest that a minimum of 5 mm of bone should exist
between the edge of a bony defect and the incision
4. Avoid incisions across major muscle attachments
Repositioning difficult delayed healing and scar formation
5. Tissue retractor should rest on solid bone
Access impaired
Trauma to mucosal tissues
Lubow RM, Wayman BE, Cooley RL. Endodontic flap design: analysis and recommendations for current usage. Oral Surgery, Oral Medicine, Oral Pathology.
9.
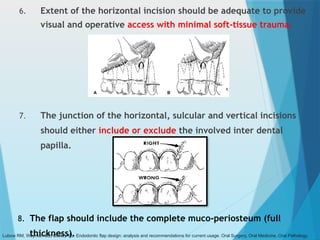
6. Extent ofthe horizontal incision should be adequate to provide
visual and operative access with minimal soft-tissue trauma.
7. The junction of the horizontal, sulcular and vertical incisions
should either include or exclude the involved inter dental
papilla.
8. The flap should include the complete muco-periosteum (full
thickness).
Lubow RM, Wayman BE, Cooley RL. Endodontic flap design: analysis and recommendations for current usage. Oral Surgery, Oral Medicine, Oral Pathology.
10.
CLASSIFICATION
Various classifications arein circulation but the main criteria for a
classification should be simple of understanding of the salient
differentiating features amongst the various entities.
For easy clinical application three parameters are important.
The anatomical
position of the
incision
The number of
vertical
incisions in a
flap
The shape of
the flap
Newman MG, Takei H, Klokkevold PR, Carranza FA. Newman and Carranza's Clinical periodontology. Elsevier Health Sciences; 2018
11.
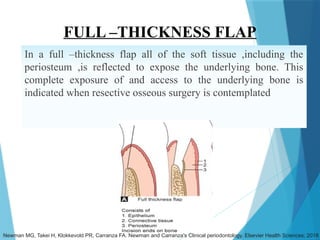
FULL –THICKNESS FLAP
Ina full –thickness flap all of the soft tissue ,including the
periosteum ,is reflected to expose the underlying bone. This
complete exposure of and access to the underlying bone is
indicated when resective osseous surgery is contemplated
Newman MG, Takei H, Klokkevold PR, Carranza FA. Newman and Carranza's Clinical periodontology. Elsevier Health Sciences; 2018
12.
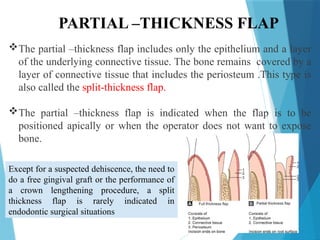
PARTIAL –THICKNESS FLAP
Thepartial –thickness flap includes only the epithelium and a layer
of the underlying connective tissue. The bone remains covered by a
layer of connective tissue that includes the periosteum .This type is
also called the split-thickness flap.
The partial –thickness flap is indicated when the flap is to be
positioned apically or when the operator does not want to expose
bone.
Except for a suspected dehiscence, the need to
do a free gingival graft or the performance of
a crown lengthening procedure, a split
thickness flap is rarely indicated in
endodontic surgical situations
13.
Full Mucoperiosteal flapLimited Mucoperiosteal
flap
Triangular -1 vertical relieving incision Sub marginal
curved/ semilunar
Rectangular -2 vertical relieving incisions Submarginal rectangular (leubke-ochsenbein)
Horizontal -No vertical relieving incision Muco gingival flap
Trapezoidal - broad based flap
According to Gutmann and Harrison
14.
According to Franklin.S.Weine
Semilunar
Full vertical
Leubke-Oschenbein
This grouping of flaps is not based on any criteria and does not include all the
flaps existing currently.
It does not give information about the anatomical position of the incision,
number of vertical incisions or about the shape of the flap.
Thus, this classification is not followed widely.
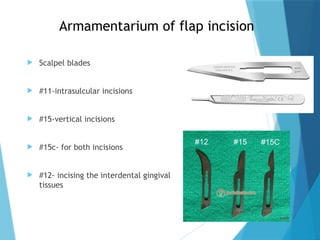
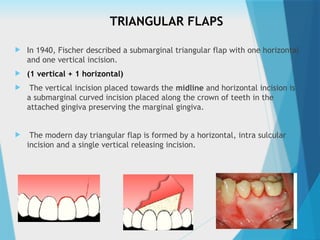
TRIANGULAR FLAPS
In1940, Fischer described a submarginal triangular flap with one horizontal
and one vertical incision.
(1 vertical + 1 horizontal)
The vertical incision placed towards the midline and horizontal incision is
a submarginal curved incision placed along the crown of teeth in the
attached gingiva preserving the marginal gingiva.
The modern day triangular flap is formed by a horizontal, intra sulcular
incision and a single vertical releasing incision.
19.
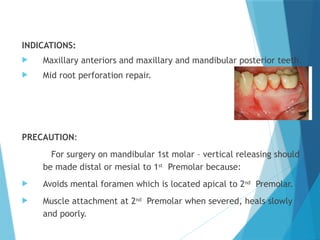
INDICATIONS:
Maxillary anteriorsand maxillary and mandibular posterior teeth.
Mid root perforation repair.
PRECAUTION:
For surgery on mandibular 1st molar – vertical releasing should
be made distal or mesial to 1st
Premolar because:
Avoids mental foramen which is located apical to 2nd
Premolar.
Muscle attachment at 2nd
Premolar when severed, heals slowly
and poorly.
20.
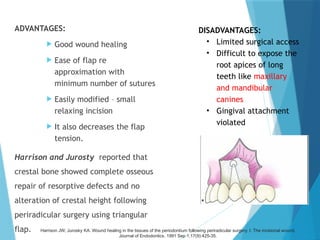
ADVANTAGES:
Good woundhealing
Ease of flap re
approximation with
minimum number of sutures
Easily modified – small
relaxing incision
It also decreases the flap
tension.
Harrison and Jurosty reported that
crestal bone showed complete osseous
repair of resorptive defects and no
alteration of crestal height following
periradicular surgery using triangular
flap.
DISADVANTAGES:
• Limited surgical access
• Difficult to expose the
root apices of long
teeth like maxillary
and mandibular
canines
• Gingival attachment
violated
Harrison JW, Jurosky KA. Wound healing in the tissues of the periodontium following periradicular surgery. I. The incisional wound.
Journal of Endodontics. 1991 Sep 1;17(9):425-35.
21.
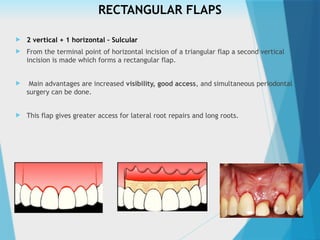
RECTANGULAR FLAPS
2vertical + 1 horizontal – Sulcular
From the terminal point of horizontal incision of a triangular flap a second vertical
incision is made which forms a rectangular flap.
Main advantages are increased visibility, good access, and simultaneous periodontal
surgery can be done.
This flap gives greater access for lateral root repairs and long roots.
22.
INDICATIONS:
Mandibular Anteriors
Multiple teeth
Teeth with long roots like maxillary canines
Lateral root repairs.
Large lesions
CONTRAINDICATION :
• Posterior teeth
ADVANTAGES:
• Increased surgical
access to root apex
• Reduces retraction
tension
• Facilitates
repositioning
DISADVANTAGES:
• Post surgical stabilization is
difficult (As the flap tissues
are held in position only by
sutures)
• Gingival attachment violated –
recession, crestal bone loss
and dehiscence.
23.
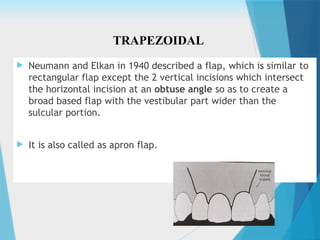
Neumann andElkan in 1940 described a flap, which is similar to
rectangular flap except the 2 vertical incisions which intersect
the horizontal incision at an obtuse angle so as to create a
broad based flap with the vestibular part wider than the
sulcular portion.
It is also called as apron flap.
TRAPEZOIDAL
24.
Disadvantage
Compromise inblood supply
The angulated vertical incision makes the unflapped tissue deprived of
adequate blood supply and leads to sloughing.
This in turn may lead to tearing out of sutures.
Delayed wound healing by secondary intention.
Soft tissue clefting or pockets could result when a dehiscence is uncovered
.
25.
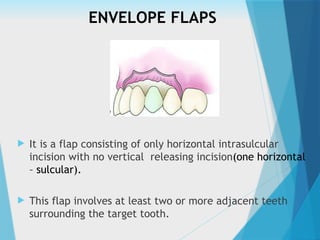
ENVELOPE FLAPS
Itis a flap consisting of only horizontal intrasulcular
incision with no vertical releasing incision(one horizontal
– sulcular).
This flap involves at least two or more adjacent teeth
surrounding the target tooth.
26.
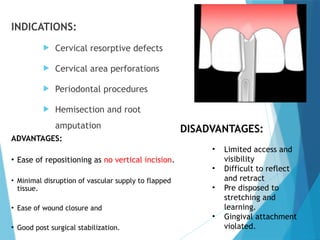
INDICATIONS:
Cervical resorptivedefects
Cervical area perforations
Periodontal procedures
Hemisection and root
amputation
ADVANTAGES:
• Ease of repositioning as no vertical incision.
• Minimal disruption of vascular supply to flapped
tissue.
• Ease of wound closure and
• Good post surgical stabilization.
DISADVANTAGES:
• Limited access and
visibility
• Difficult to reflect
and retract
• Pre disposed to
stretching and
learning.
• Gingival attachment
violated.
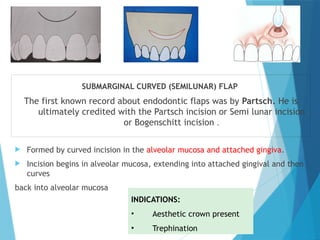
SUBMARGINAL CURVED (SEMILUNAR)FLAP
The first known record about endodontic flaps was by Partsch. He is
ultimately credited with the Partsch incision or Semi lunar incision
or Bogenschitt incision .
Formed by curved incision in the alveolar mucosa and attached gingiva.
Incision begins in alveolar mucosa, extending into attached gingival and then
curves
back into alveolar mucosa
INDICATIONS:
• Aesthetic crown present
• Trephination
29.
ADVANTAGES:
Maintains integrityof
gingival attachment
Reduces incision and
reflection time
Eliminates potential
crestal bone loss
DISADVANTAGES:
• Poor surgical access
• Poor wound healing – scaring
• Increased haemorrhage
• Crosses root eminences
• Predisposed to stretching and
tearing
• Difficult to reposition
30.
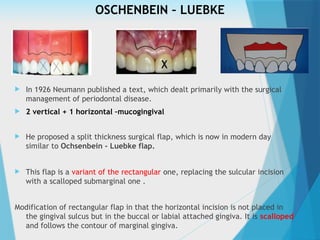
OSCHENBEIN – LUEBKE
In 1926 Neumann published a text, which dealt primarily with the surgical
management of periodontal disease.
2 vertical + 1 horizontal –mucogingival
He proposed a split thickness surgical flap, which is now in modern day
similar to Ochsenbein - Luebke flap.
This flap is a variant of the rectangular one, replacing the sulcular incision
with a scalloped submarginal one .
Modification of rectangular flap in that the horizontal incision is not placed in
the gingival sulcus but in the buccal or labial attached gingiva. It is scalloped
and follows the contour of marginal gingiva.
32.
INDICATIONS :
• Prostheticcrowns
• Periradicular surgery of anterior region, longer roots
• Wide band of attached gingiva with proper re appoximation and
good soft tissue management
Horizontal incision runs along attached gingiva following the gingival
scallops.
In order to avoid dehiscences and gum recessions incision should not
involve the gingival sulcus nor the junctional epithelium but should
run between the bone margin and the mucogingival line.
33.
Disadvantage
An unaestheticscar may form.
Muscle attachments and frenum
present anatomic obstructions and
hinders the reflection of flap.
This flap is essentially limited only
to maxillary anteriors and posteriors.
It is not used in mandibular
anteriors because the tissue in this
region is thin and friable and wound
closure is difficult.
Advantage
Provides good access,
Does not involve marginal
gingiva so crestal bone loss is
not seen
This flap is indicated in
presence of prosthetic crowns
and existing non pathogenic
dehiscence are avoided
34.
FEATURES
Purpose ofscalloped incision is to provide guide for correct
repositioning of flap for suturing.
The angle of incision in relation to cortical plate is 45o _
provides
the widest cut surface allowing better flap repositioning
The vertical incision should be straight up and down following
fiber lines in the mucosa
The junction where horizontal scalloped incision meets the
vertical incision should be rounded to promote faster and
smoother healing. If 90o
, it heals slowly and leaves small hard,
knobby scar.
35.
ADVANTAGES:
Does notinvolve marginal
and inter dental gingiva
Crestal bone not exposed
Enhanced visibility and
access
Ease in repositioning
Avoids dehiscence
DISADVANTAGES:
Vertically oriented
blood vessels and
collagen fibres are
severed – increased
bleeding, shrinkage,
scaring and delayed
healing.
36.
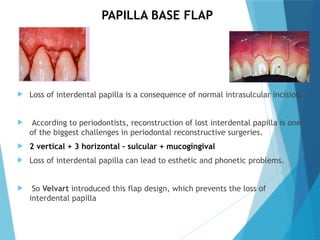
PAPILLA BASE FLAP
Loss of interdental papilla is a consequence of normal intrasulcular incision.
According to periodontists, reconstruction of lost interdental papilla is one
of the biggest challenges in periodontal reconstructive surgeries.
2 vertical + 3 horizontal – sulcular + mucogingival
Loss of interdental papilla can lead to esthetic and phonetic problems.
So Velvart introduced this flap design, which prevents the loss of
interdental papilla
37.
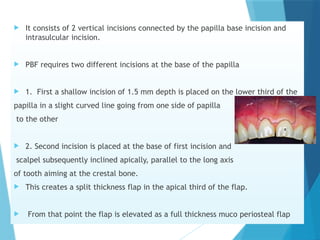
It consistsof 2 vertical incisions connected by the papilla base incision and
intrasulcular incision.
PBF requires two different incisions at the base of the papilla
1. First a shallow incision of 1.5 mm depth is placed on the lower third of the
papilla in a slight curved line going from one side of papilla
to the other
2. Second incision is placed at the base of first incision and
scalpel subsequently inclined apically, parallel to the long axis
of tooth aiming at the crestal bone.
This creates a split thickness flap in the apical third of the flap.
From that point the flap is elevated as a full thickness muco periosteal flap
38.
ADVANTAGES
Absence ofgingival
recession
Absence of papilla
retraction,
Almost complete absence
of scars
It also guarantees a large
surgical area exposition
without flap stretching,
also permitting periapical
surgery on long roots.
DISADVANTAGES
Two different incisions are needed
to achieve good healing which makes
the flap design technique sensitive.
Proper attention should be given not
to undermine the flap and make it
thin, which leads to difficulty in
handling the flap
More number of sutures are needed
Even though no inter dental papillary
recession is not present, there is mild
recession in the cervical area of the
flap.
39.
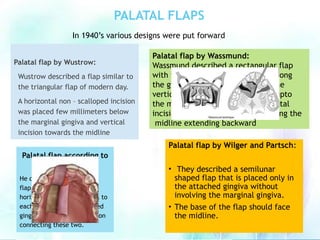
PALATAL FLAPS
Palatal flapby Wustrow:
Wustrow described a flap similar to
the triangular flap of modern day.
A horizontal non – scalloped incision
was placed few millimeters below
the marginal gingiva and vertical
incision towards the midline
Palatal flap by Wassmund:
Wassmund described a rectangular flap
with two horizontal incisions one along
the gingival crevice of tooth and one
vertical incision made just before upto
the midline, then the other horizontal
incision parallel to the first one along the
midline extending backward
Palatal flap by Wilger and Partsch:
• They described a semilunar
shaped flap that is placed only in
the attached gingiva without
involving the marginal gingiva.
• The base of the flap should face
the midline.
Palatal flap according to
Fischer:
He described a rectangular
flap with two nonscalloped
horizontal incisions parallel to
each other made in attached
gingiva and a vertical incision
connecting these two.
In 1940’s various designs were put forward
40.
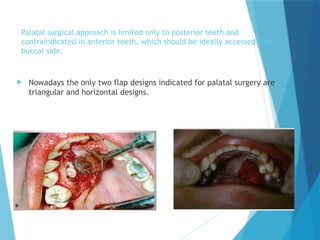
Palatal surgical approachis limited only to posterior teeth and
contraindicated in anterior teeth, which should be ideally accessed from
buccal side.
Nowadays the only two flap designs indicated for palatal surgery are
triangular and horizontal designs.
41.
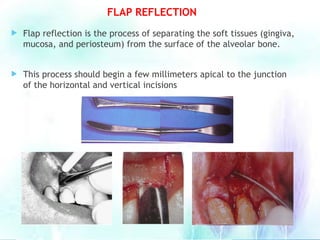
FLAP REFLECTION
Flapreflection is the process of separating the soft tissues (gingiva,
mucosa, and periosteum) from the surface of the alveolar bone.
This process should begin a few millimeters apical to the junction
of the horizontal and vertical incisions
42.
It isintiated from the vertical incision in attached gingiva
Periosteal elevator is used to apply reflective forces, elevating the
periosteum and its superficial tissues from the cortical plate.
Elevator is then directed coronally , allowing the marginal and interdental
gingiva to be lifted from their opposing incisional wound edges without the
direct application of damaging forces.
All reflective forces are applied to the periosteum and as the periosteum is
lifted from crestal bone, the incised supracrestal attached gingiva, marginal
gingiva and interdental gingiva are passively reflected with base of the flap.
43.
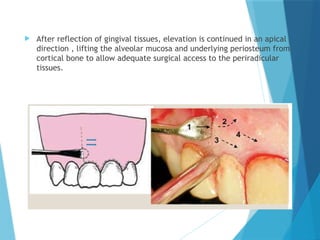
After reflectionof gingival tissues, elevation is continued in an apical
direction , lifting the alveolar mucosa and underlying periosteum from
cortical bone to allow adequate surgical access to the periradicular
tissues.
44.
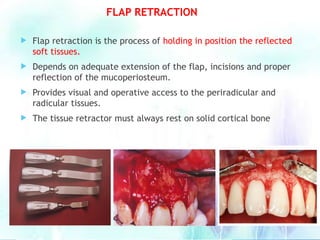
Flap retractionis the process of holding in position the reflected
soft tissues.
Depends on adequate extension of the flap, incisions and proper
reflection of the mucoperiosteum.
Provides visual and operative access to the periradicular and
radicular tissues.
The tissue retractor must always rest on solid cortical bone
FLAP RETRACTION
45.
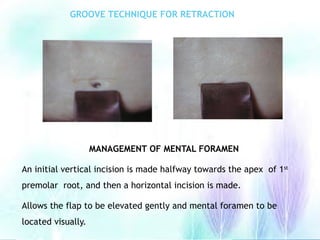
GROOVE TECHNIQUE FORRETRACTION
MANAGEMENT OF MENTAL FORAMEN
An initial vertical incision is made halfway towards the apex of 1st
premolar root, and then a horizontal incision is made.
Allows the flap to be elevated gently and mental foramen to be
located visually.
46.
PRECAUTIONS:
Longer theflap retracted, greater the post surgical morbidity
Reduced blood supply
Hypoxia and acidosis
Delayed healing
Limited mucoperiosteal flaps are susceptible to dehydration and
hence require frequent irrigation compared to full mucoperiosteal
flaps
47.
TIME OF RETRACTION
An axiomatic principle of surgery is that the longer the flap is reflected , the
greater the complication following surgery
Because vascular flow is undoubtedly impeded during retraction and at some
point in time , tissue hypoxia and acidosis will result in damage which may
delay wound healing.
Whether the reflection time is short or long ,flaps should be irrigated
frequently during surgical procedures to prevent dehydration of the
periosteal surfaces of flap.
Because of severance of the vertically oriented supraperiosteal vessels ,limited
mucoperiosteal flaps are likely more susceptible to dehydration and may
require more frequent irrigation than full mucoperiosteal flap.
48.
Healing
Oral mucosa ischaracterised by a cell turnover much faster than
other tissues, among the causes endothelial growth factors like the
VEGF, which can start the angiogenesis, has high relevance.
Within 24 hours a complex process characterised of several phases
bringing to the healing of the treated tissue starts.
Leukocytes and macrophages start moving in the blood toward the
wound. Inflammation and repairing cells reach the area through
the fibrin layers supported by the microvascularization of the flap
and the underlying tissue.
49.
In theprocess of re-epitheliation the integrins have a very
important role; these surface proteins regulate the growth,
diversification and the immune response functions of the cell
by picking up information from the extracellular matrix and
connecting through exchanges of information with the
internal side of the cell
• Under this action, the margins of the flap start migrating
to cover the underlying connecting tissue.
• The keratinocytes that cover the connective tissue are
phagocytes able to enter the fibrin layer, remove it and
generate through integrins and eventually generate a new
basal membrane.
50.
Cells thenorganise themselves creating a layer of two to three cells
called basal layer which is the germinative state of epithelial cells.
This phase lasts one to two days depending on the distance between the
two flaps.
Approximately on the seventh day, the epithelium matures in several
layers while the corneal layer becomes evident.
In contrast the healing of the connective tissue takes longer than the
epithelial tissue; in fact the process develops through the generation of
the granulation tissue, followed by a phase of reorganisation, contraction
and eventual remodelling of the tissue.
The reparative process is managed by fibroblasts that are subject to a
series of changes making them the main contributors to the healing
process.
51.
For the correcthealing some precaution
avoid unpleasant scars in the area
surgically treated:
The haematic flux of the flap should not be altered.
The wound must be irrigated with saline solution to
keep the tissue humid
Trying to remove the fibrous parts which would impede
the first intention healing
In patientswith healthy marginal periodontal conditions, the PBI
allows rapid and predictable recession-free healing, whereas
complete mobilization of the papilla led to a marked loss of the
papilla height. In aesthetically relevant areas, the use of the PBI is
recommended, to avoid opening of the interproximal space, when
periradicular surgical treatment is necessary.
Velvart P
, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular
full-thickness flap and papilla base flap in endodontic surgery.Int Endod J. 2019
Oct;36(10):653–9.
AIM:
To compare the loss of papilla height when using the papilla base
incision (PBI) or the standard papilla mobilization incision in marginal
full-thickness flap in cases with no evidence of marginal
periodontitis.
54.
Healing following apicalsurgeries depend a large
extent on the soft tissue flap design. Different flap
designs have been advocated and used, depending
on the location and size of the peri-radicular lesion.
A new flap design, which used sub-marginal straight
incision was compared with intra-sulcular
rectangular/triangular flap and scalloped sub-
marginal flap. Post - Operative healing was
compared for swelling, alternation of colour,
recession of marginal gingival and extent of scarring.
It was found that sub-marginal straight horizontal
incision showed better healing with lesser
scarring. It is concluded that the new flap design
can provide an alternative.
KK W, Garg A. Healing of soft tissue after different types of flap designs used in
periapical surgery. Endodontology. 2004;16.
55.
In thisstudy; Ocshenbein-Leubke (OL) and trapezoidal (TZ) flaps have been
compared in terms of their efficacy and comfort.
OL flap was found to be better than TZ flap with respect to time of flap
reflection, accessibility, duration of surgery and post-operative pain. The OL
flap takes less time for reflection with nearly the same accessibility, less
post-operative pain and less complication as compared to TZ flap. They
conclude that OL flap gives better results when compared to TZ flap.
Ahmed MV, Rastogi S, Baad RK, Gupta AK, Nishad SG, Bansal M, Kumar S, Oswal R, Mahendra
P, Bhatnagar A. Comparative Study Between Two Flaps—Trapezoidal flap (TZF) and
Ocshenbein-Leubke Flap (OLF) in Periapical Surgeries. Journal of maxillofacial and oral
surgery. 2013 Dec 1;12(4):440-6.
56.
Use of partial-thicknessflaps does not prevent from all bone
loss. The procedure may result most of the times in less bone
loss than the elevation of full-thickness flaps. Further
research has to evaluate the determinants of effective
outcomes of partial-thickness flap procedures.
Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB. Bone
loss after full‐thickness and partial‐thickness flap elevation. Journal of clinical
periodontology. 2011 Feb;38(2):157-62.
57.
CONCLUSION
Designing theflap is a key aspect of periapical surgery.
It should ensure adequate exposure of the surgical field and allow the surgeon to
work quickly and comfortably.
Futhermore , there should be no tension capable of complicating the work of the
dental professional or of causing patient discomfort , and soft tissue damage due to
retractor compression is to be avoided.
A good flap design with delicate manipulation of the soft tissue is necessary for
successful periapical surgery.
58.
REFERENCES
Surgical endodontics–JAMES GUTTMAN
Grossman’s endodontic practice –B. suresh chandra V.Gopikrishna-13th
edition
Cecchetti F, Ricci S, Di Giorgio G, Pisacane C, Ottria L. Microsurgery flap in endodontic surgery:
case report. ORAL & implantology. 2018 Jan;2(1):19.edition
Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-
thickness flap and papilla base flap in endodontic surgery.Int Endod J. 2015 Oct;36(10):653–9.
KK W, Garg A. Healing of soft tissue after different types of flap designs used in periapical surgery.
Endodontology. 2004;16.
Grandi C, Pacifici L. The ratio in choosing access flap for surgical endodontics: a review. ORAL &
implantology. 2009 Jan;2(1):37.
Ahmed MV, Rastogi S, Baad RK, Gupta AK, Nishad SG, Bansal M, Kumar S, Oswal R, Mahendra P,
Bhatnagar A. Comparative Study Between Two Flaps—Trapezoidal flap (TZF) and Ocshenbein-
Leubke Flap (OLF) in Periapical Surgeries. Journal of maxillofacial and oral surgery. 2013 Dec
1;12(4):440-6.
Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB. Bone loss after full‐
thickness and partial thickness flap elevation. Journal of clinical periodontology.2018
‐
59.
Grandi C,Pacifici L. The ratio in choosing access flap for surgical
endodontics: a review. ORAL & implantology. 2009 Jan;2(1):37.
Ahmed MV, Rastogi S, Baad RK, Gupta AK, Nishad SG, Bansal M, Kumar S,
Oswal R, Mahendra P, Bhatnagar A. Comparative Study Between Two Flaps
—Trapezoidal flap (TZF) and Ocshenbein-Leubke Flap (OLF) in Periapical
Surgeries. Journal of maxillofacial and oral surgery. 2013 Dec 1;12(4):440-
6.
Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB.
Bone loss after full‐thickness and partial‐thickness flap elevation. Journal
of clinical periodontology. 2011 Feb;38(2):157-62.
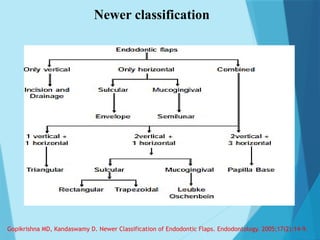
Gopikrishna MD, Kandaswamy D. Newer Classification of Endodontic
Flaps. Endodontology. 2005;17(2):14-9.
#5 FLAP
Developed to gain access to surgical sites or to move tissue from one place to another
#6 To manage the various complications and to achieve unimpeded access a full mucoperiosteal flap or a split thickness flap should be elevated.
#12 To manage the various complications and to achieve unimpeded access a full mucoperiosteal flap or a split thickness flap should be elevated.
#31 2 vertical + 1 horizontal –mucogingival
Modification of rectangular flap in that the horizontal incision is not placed in the gingival sulcus but in the buccal or labial attached gingiva. It is scalloped and follows the contour of marginal gingiva
#39 Wassmund described a rectangular flap with two horizontal incisions one along the gingival crevice of tooth and one vertical incision made just before upto the midline, then the other horizontal incision parallel to the first one along the
midline extending backward
He described a rectangular flap with two nonscalloped horizontal incisions parallel to each other made in attached gingiva and a vertical incision connecting these two.
#57 The endodontic surgeon must understand that:-
All flap designs have both advantages and disadvantages.
No single flap design is amenable to all surgical cases.
#60 A flap is defined as a section of gingiva and or mucosa surgically elevated from the underlying tissues to provide visibility and access to the bone and root surface
Full thickness epithelium ct periostem




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



