


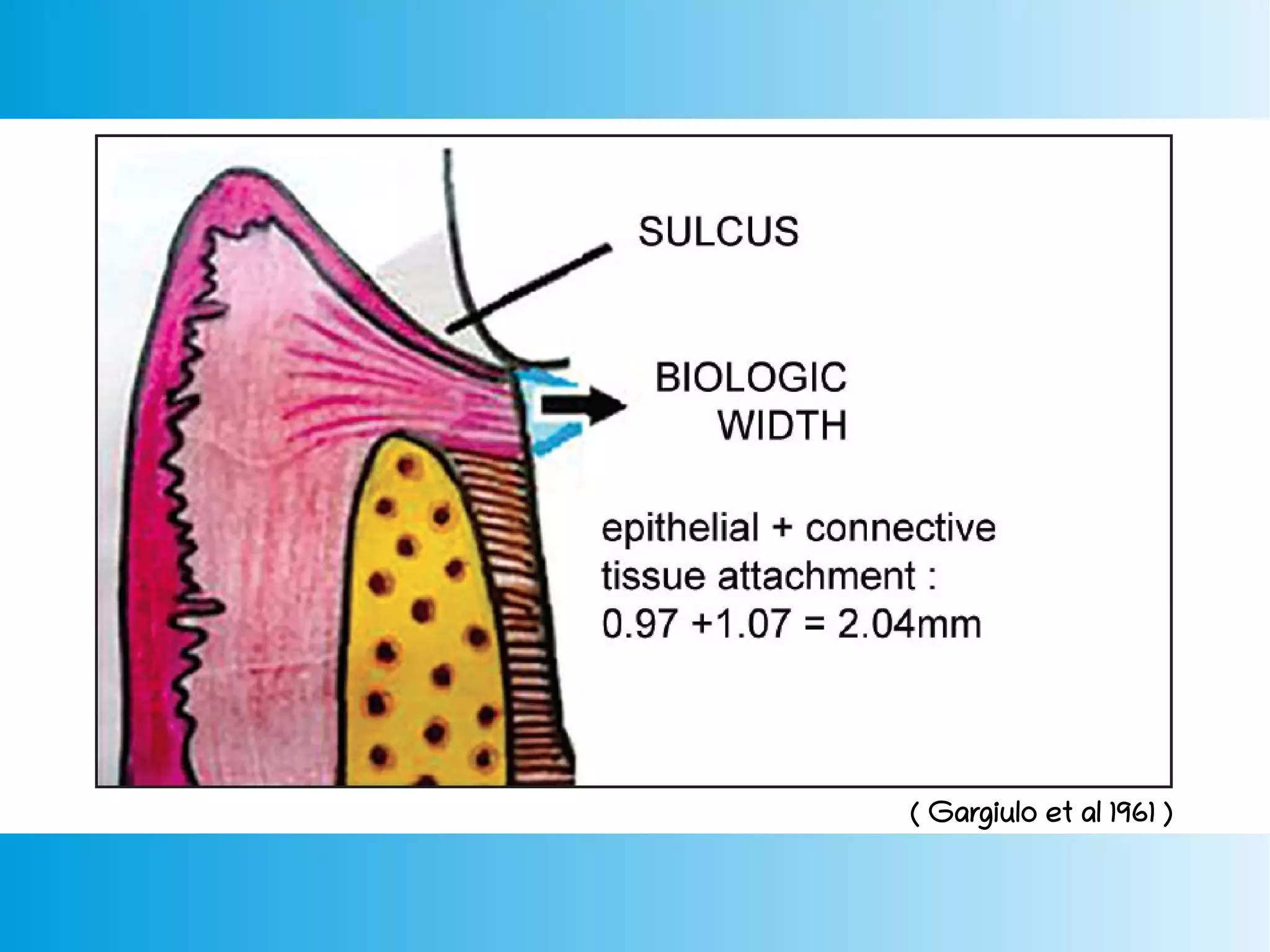

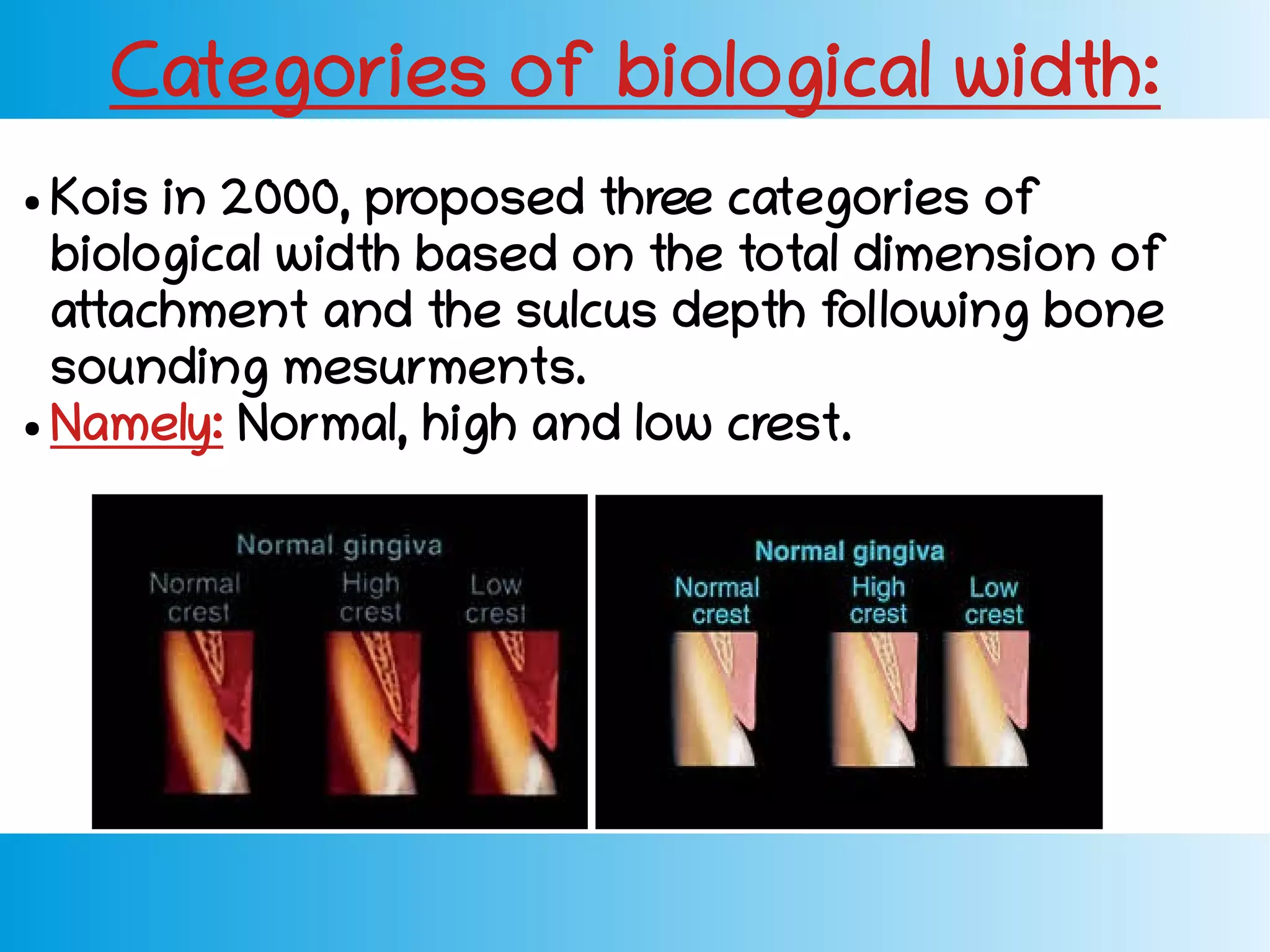




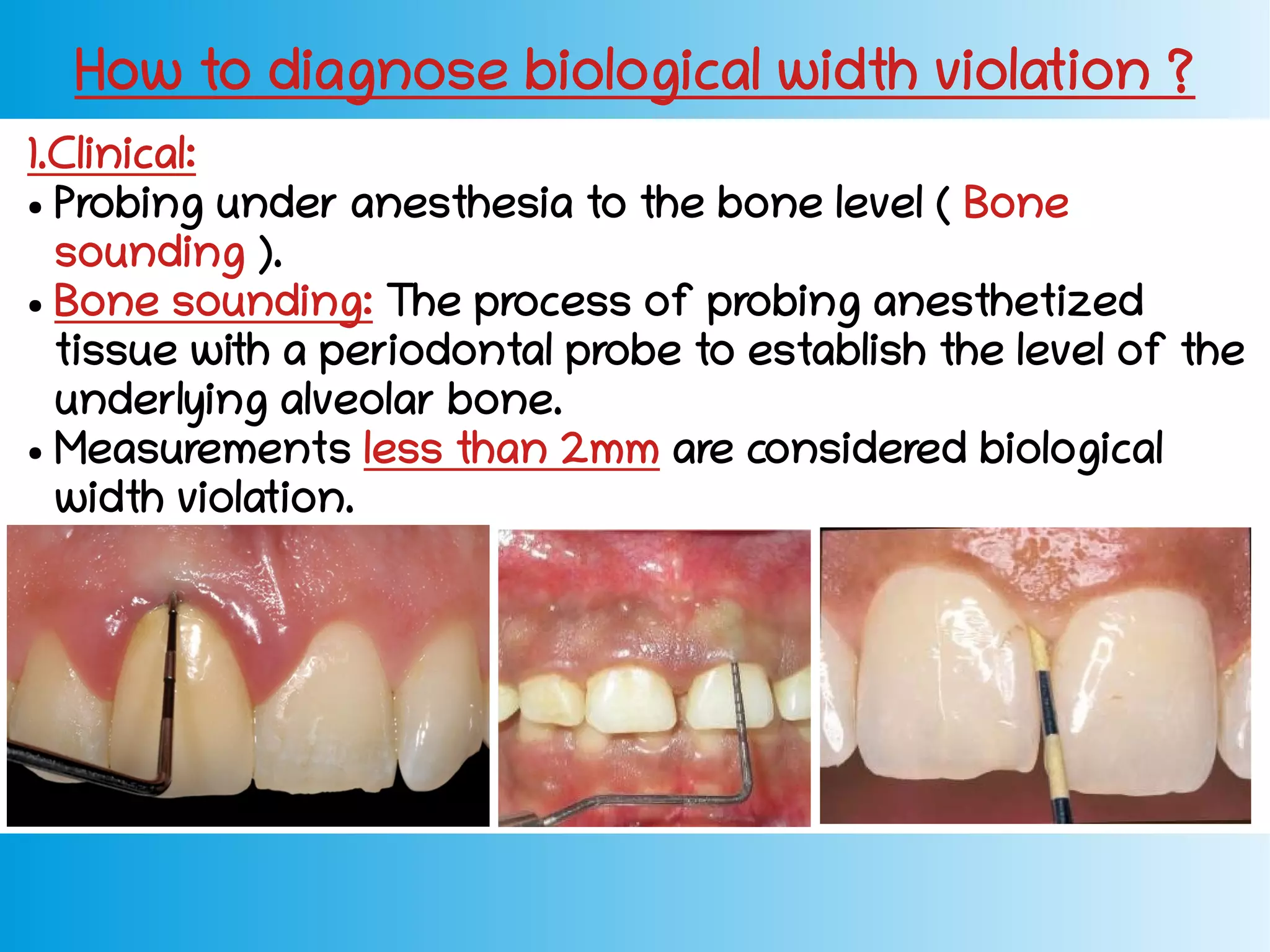









This document discusses biological width, which refers to the dimension of soft tissue attached to the tooth above the alveolar bone crest. It includes the junctional epithelium and connective tissue attachment. The total biological width in healthy tissue is about 2.04mm. Violation of the biological width due to factors like poor oral hygiene, defective restorations, or over-contouring can lead to inflammation and bone loss. Diagnosis involves probing measurements and radiographs. Biological width can be restored through surgical crown lengthening or orthodontic extrusion procedures.



































































