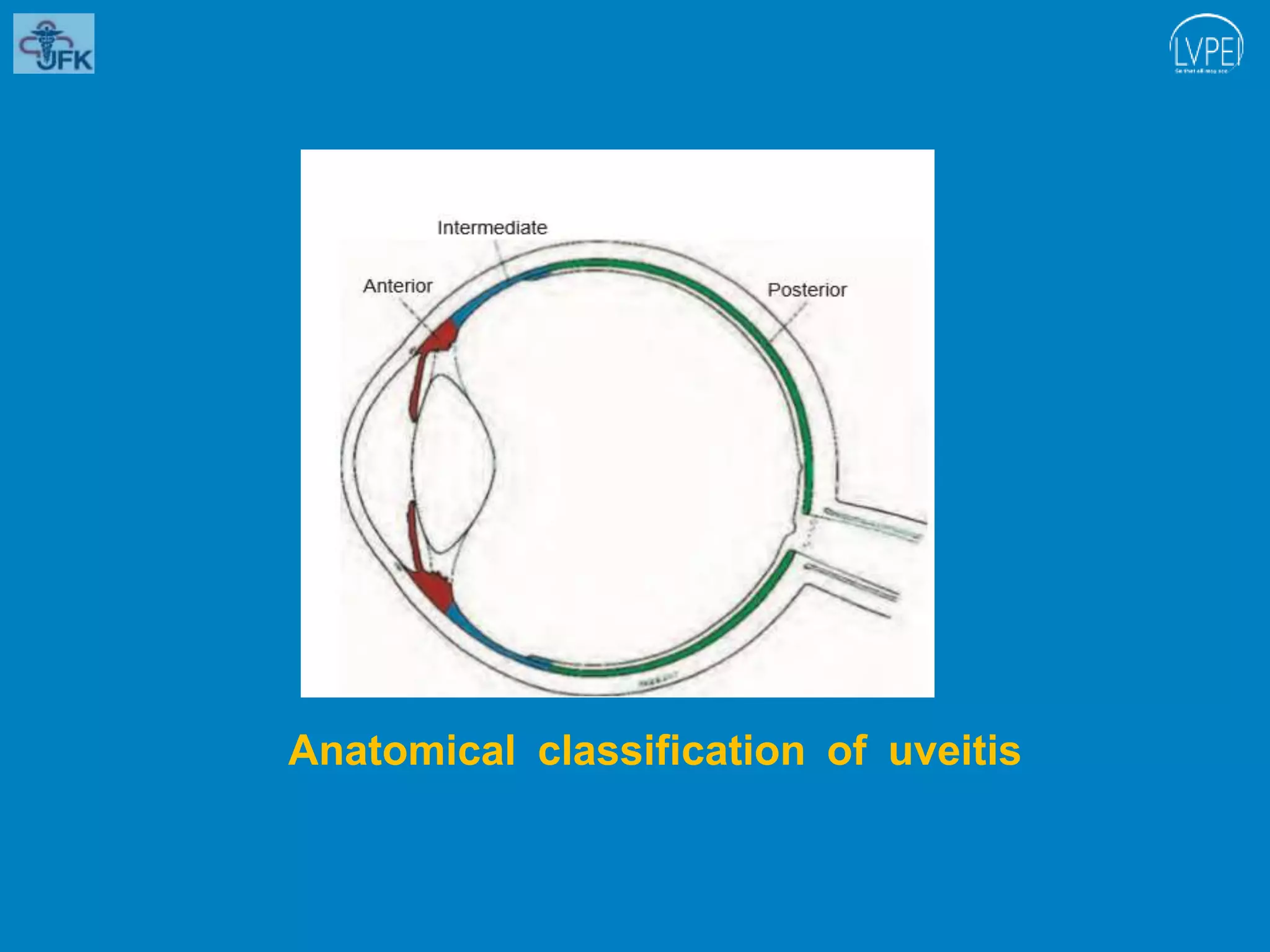
The document discusses uveitis, an inflammation of the uveal tract of the eye, outlining its classification, clinical features, and symptoms. It describes various forms of uveitis based on anatomical location, clinical course, and pathology, emphasizing the characteristics of anterior, intermediate, and posterior uveitis. The document also details related symptoms, including pain, visual disturbances, and specific ocular signs associated with inflammation.