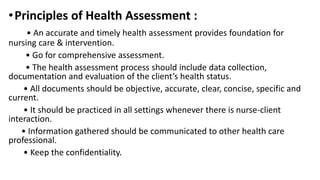
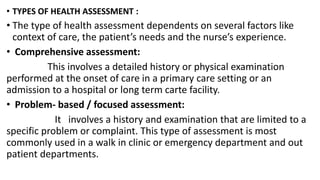
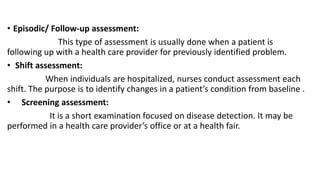
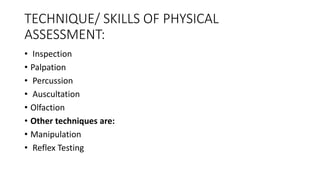
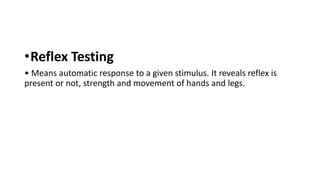
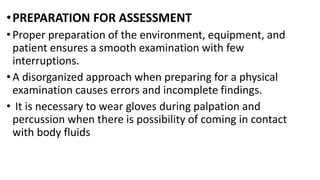
This document discusses health assessment for nursing. It defines health assessment as a systematic appraisal of all factors relevant to a client's health that provides the foundation for quality nursing care. The purposes of health assessment include gathering baseline health data, confirming diagnoses, and evaluating care outcomes. The principles of health assessment are that it should be comprehensive, accurate, and communicated between providers while maintaining confidentiality. The document outlines the techniques of health assessment including inspection, palpation, percussion, auscultation, and reflex testing. It also discusses preparing the environment, equipment, and patient for an effective health assessment.











































![✅ CCleaner Pro Free Crack 6.34 + Activation Key [APRIL-2025]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415080446-ea0ab5fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![✅ Download CCleaner Pro Key 2025 with Crack [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415082125-6d1be3de-thumbnail.jpg?width=640&height=640&fit=bounds)















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)