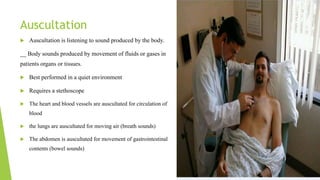
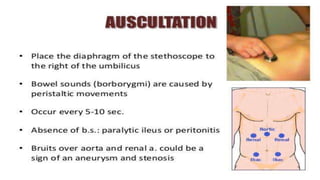
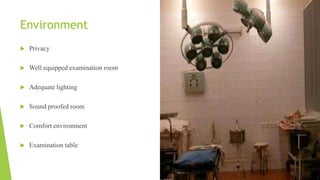
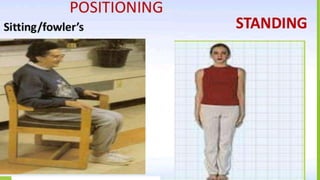
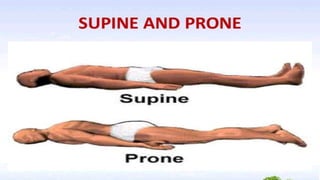
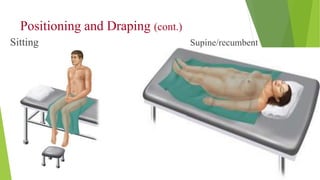
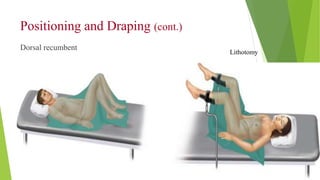
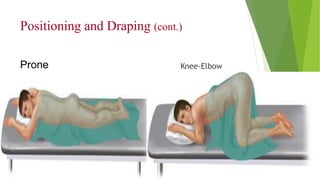
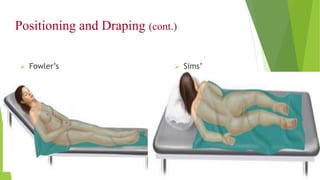
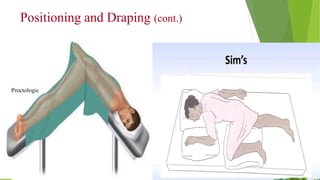
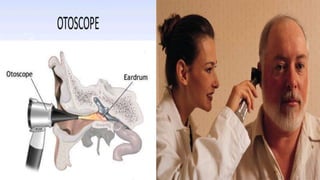
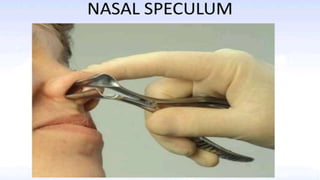
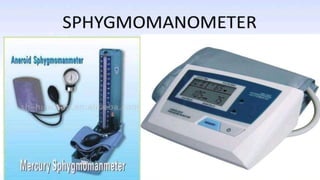
The document discusses physical assessment, which involves systematically collecting objective information about a patient through examination techniques like inspection, palpation, percussion, and auscultation. It outlines the purpose, indications, techniques, and safety precautions for each examination method. It also discusses positioning and draping patients, necessary equipment, and preparing patients for examination to make them comfortable both emotionally and physically.