Downloaded 31 times








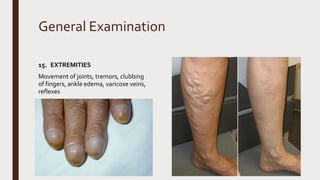
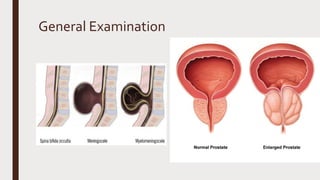
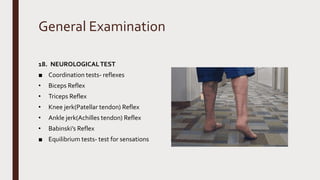


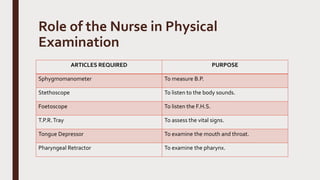
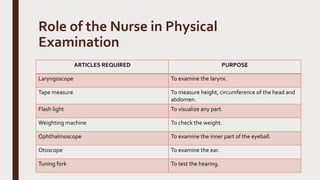
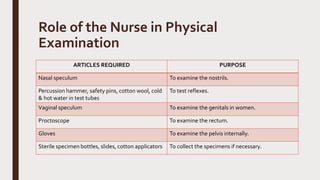

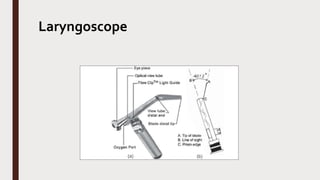






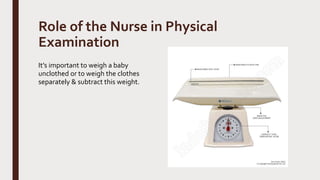

The document provides an overview of the physical assessment process. It discusses the purposes of physical assessment, which include understanding a client's physical and mental well-being, detecting diseases, determining treatment needs, and contributing to medical research. The basic techniques used in physical assessment are inspection, palpation, percussion, auscultation, manipulation, and testing of reflexes. A head-to-toe process for general examination is also outlined that covers assessment of different body systems and areas. The role of the nurse in preparing the environment, client, and necessary equipment for the physical assessment is described.











































![✅ CCleaner Pro Free Crack 6.34 + Activation Key [APRIL-2025]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415080446-ea0ab5fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![✅ Download CCleaner Pro Key 2025 with Crack [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415082125-6d1be3de-thumbnail.jpg?width=640&height=640&fit=bounds)

































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)



![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


