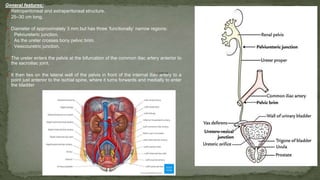
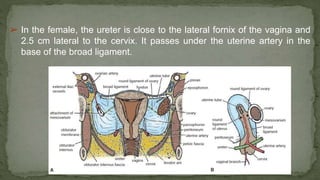
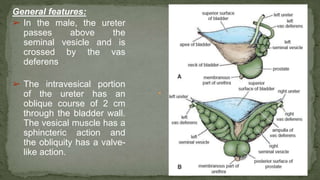
The document provides an overview of the radiological anatomy of the kidneys and adrenal glands. It describes the location, structure and blood supply of the kidneys. The document outlines the pelvicalyceal system and nephron anatomy. It also discusses congenital anomalies, imaging modalities including ultrasound, CT, MRI, and angiography. For the ureters, the document notes their course from the kidneys to the bladder and relationships in the male and female pelvis.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






