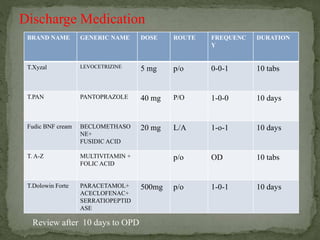
The document describes a case presentation of a 32-year-old female patient admitted with a 1.5 month history of swelling in the umbilical region. Examination revealed a 2x2 cm swelling in the umbilical region that increased in size with coughing and straining. The patient was diagnosed with an umbilical hernia and underwent surgery. Post-operatively, the patient was treated with antibiotics and pain medications and made an uneventful recovery.