Download as PDF, PPTX





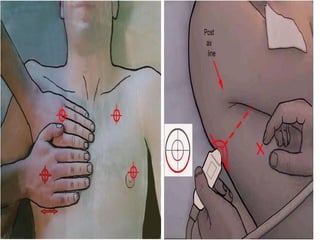
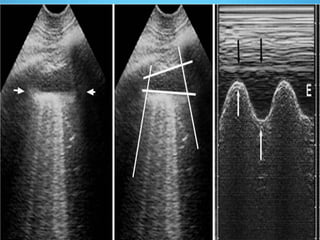
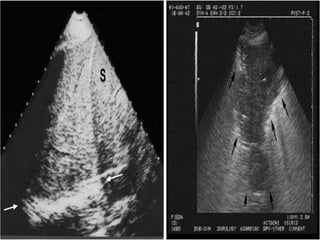
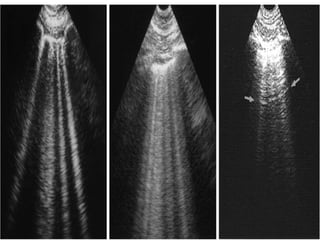
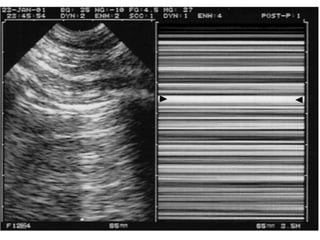
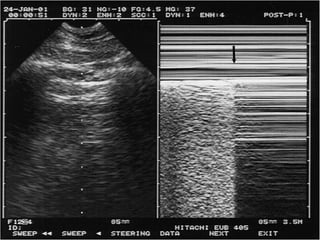

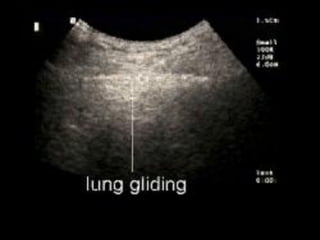

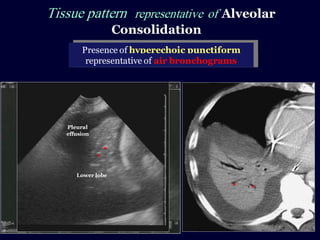

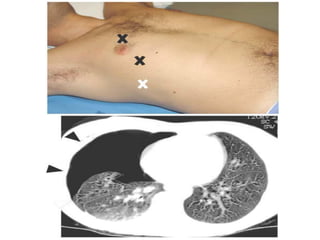

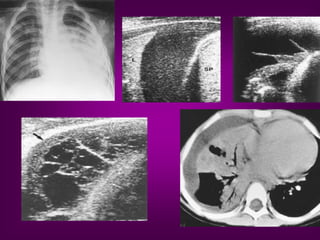

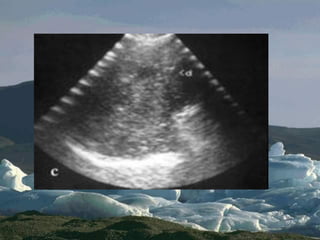
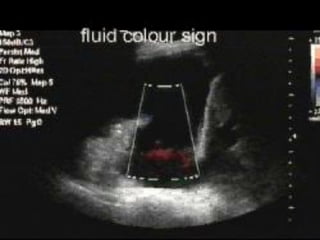

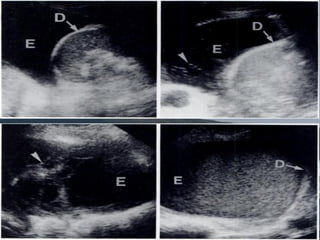
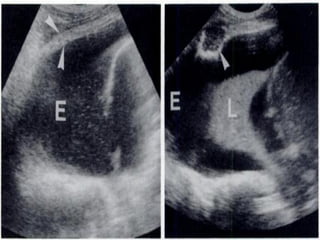
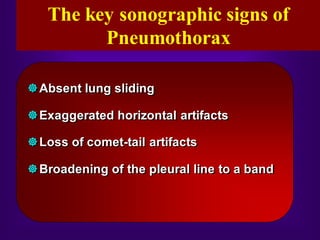


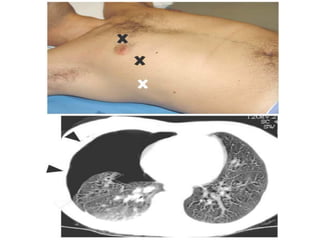
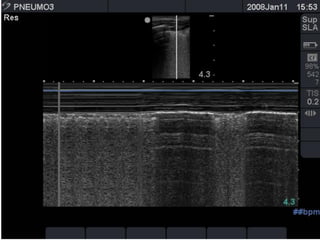
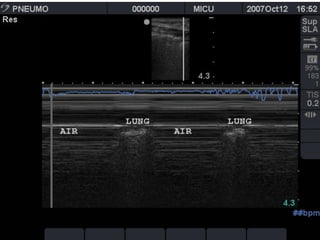
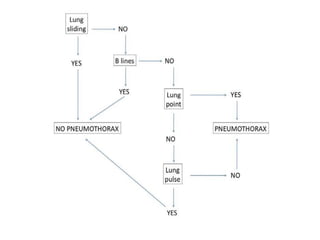
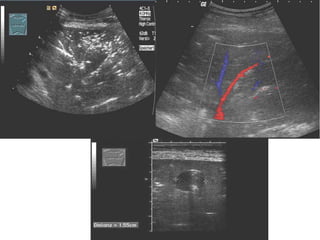

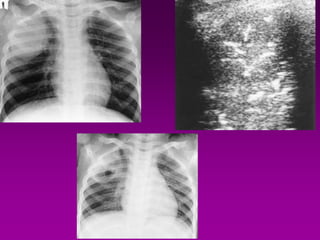
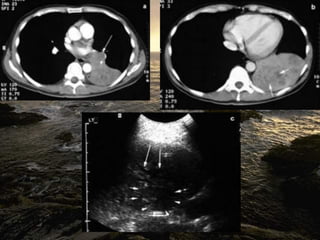
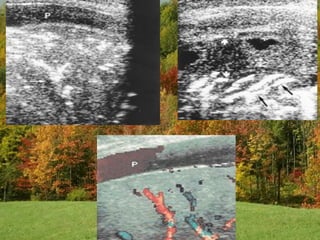
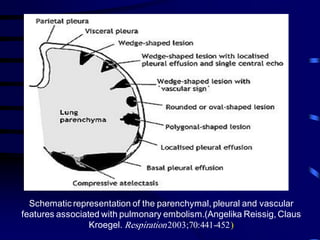
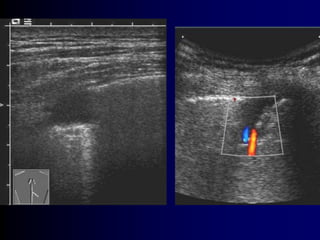


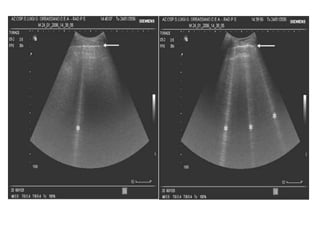

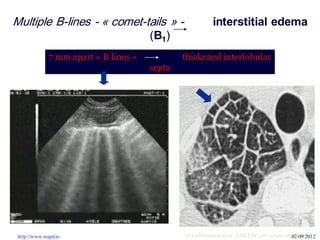
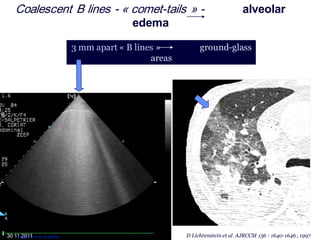
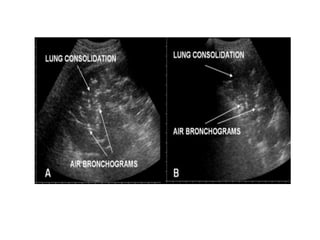
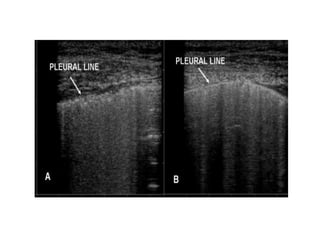

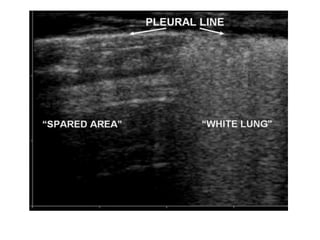
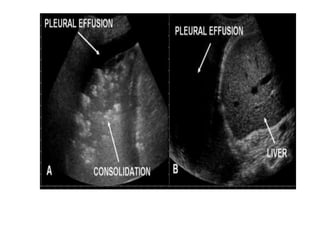



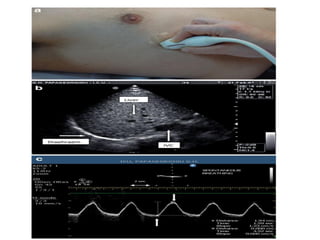

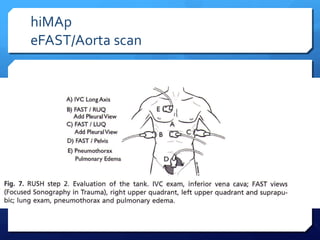
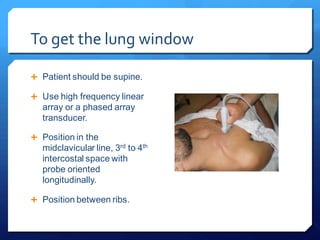
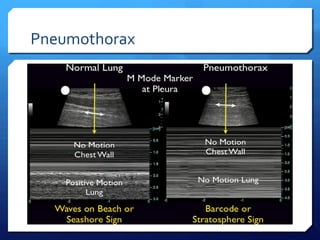
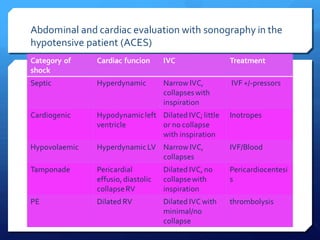
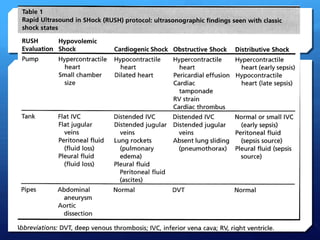





This document discusses the use of chest sonography in critically ill patients. It notes that bedside chest radiography has limitations in critically ill patients. Chest sonography can help diagnose various lung conditions at the bedside including pulmonary consolidation, atelectasis, edema, effusions, and pneumothorax. It reviews the sonographic signs and patterns associated with these conditions. The document also discusses using lung ultrasound and IVC views to assess shock states and guide treatment. Overall, it promotes the use of bedside lung ultrasound as a valuable tool to complement radiography in critically ill patients.


































































































