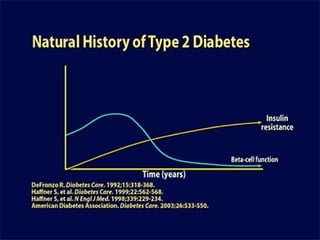
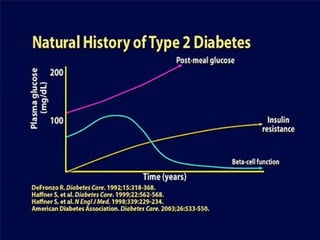
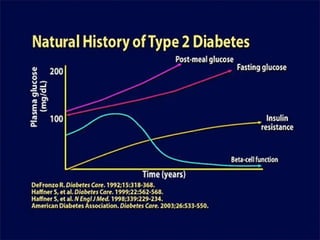
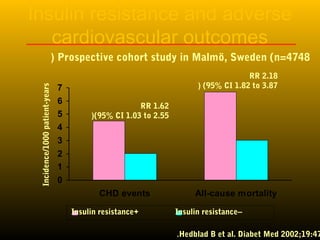
This document discusses insulin sensitizers, focusing on metformin and thiazolidinediones (TZDs). It summarizes the mechanisms of action and clinical benefits of metformin, including its cardiovascular benefits shown in UKPDS. It also discusses the mechanisms of TZDs in increasing insulin sensitivity and their role in beta cell preservation and diabetes prevention. However, it notes problems with TZDs including increased risks of heart failure, myocardial infarction and fractures that have been observed in clinical trials.


![Thiazolidinediones
• Thiazolidinediones TZDs were developed in
1997. There first member troglitazone was
withdrawn from the market in the year 2000 due
to hepatotoxicity.
• Pioglitazone and rosiglitazone appeared in the
market in 1999.
• Glitazones act predominantly by enhancing
peripheral insulin sensitivity, offering promising
perspectives in terms of β-cell preservation
[Buchanan et al, Diabetes 2002 – Ovalle and Bell, Diabetes Obes Metab
2002] and cardiovascular protection [Suwattee et al,
Endocrinologist 2002 – Dormandy et al, Lancet 2005].](https://image.slidesharecdn.com/4-ued2011metforminthegoldstandardd-150629155826-lva1-app6892/85/ued2011-metformin-the-gold-standard-d-adel-31-320.jpg)
![The Glitazones And The Beta Cell
• Beta cell failure begins more than a decade
before diabetes is diagnosed [Kahn, Cell 1998 - Donath
and Halban, Diabetologia 2004]
• Two mechanisms related to insulin resistance:
glucotoxicity, lipotoxicity.
• glitazone therapy:
- Delay or prevent beta cell failure?
- growing body of evidence that TZDs
rejuvenate beta-cells and improve their function
[Bell, Am J Med 2003].](https://image.slidesharecdn.com/4-ued2011metforminthegoldstandardd-150629155826-lva1-app6892/85/ued2011-metformin-the-gold-standard-d-adel-33-320.jpg)































![Thyroid Drugs2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroid-drugs21-1195132052359450-4-thumbnail.jpg?width=640&height=640&fit=bounds)





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)