Download to read offline


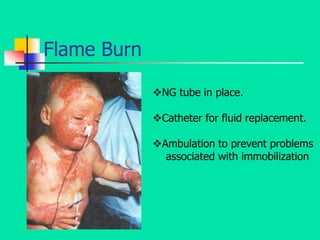
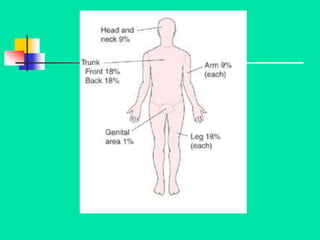





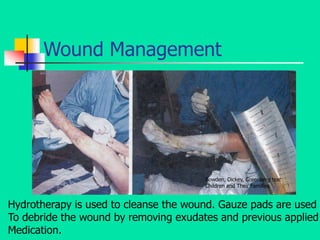


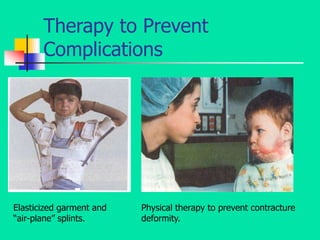


Young children are at higher risk of mortality from burns than adults due to their smaller body size and immature immune systems. Burns involving over 10% of the total body surface area require fluid resuscitation to prevent heat and fluid loss. Proper burn wound management includes cleaning, debriding dead tissue, applying ointment dressings, and skin grafts for deeper burns. Physical therapy is also important to prevent contractures and immobilization complications.




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















