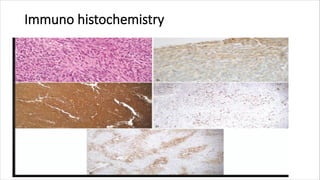
The document discusses recent advances in the understanding and classification of various epithelioid mesenchymal tumors, including epithelioid sarcoma, clear cell sarcoma, and others. Each tumor is characterized by distinct clinical presentations, microscopic features, and differential diagnoses, highlighting their associations with age, gender, and common locations. Additionally, histological and immunohistochemical characteristics are provided to assist in accurate diagnosis and treatment planning.