Downloaded 619 times


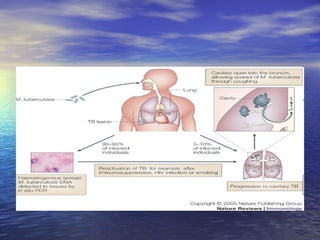


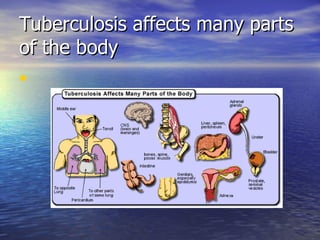







Tuberculosis is caused by the bacterium Mycobacterium tuberculosis. It affects many parts of the body and has a variable clinical presentation ranging from no symptoms to severe symptoms like fever, cough, and weight loss. Diagnosis involves tests like the tuberculin skin test and imaging tests. Treatment requires a long course of multiple anti-tuberculosis medications.








































![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
































































