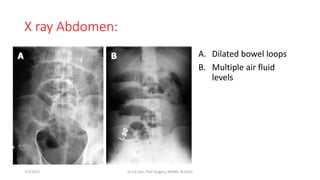
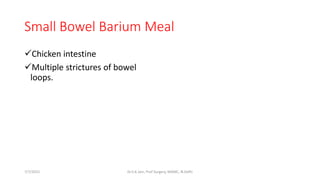
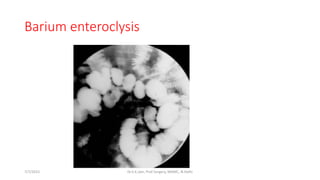
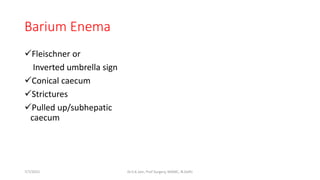
The document discusses abdominal tuberculosis, presented by Dr. Sudhir Jain. It provides background on tuberculosis, noting it was historically called "consumption" and seen as a disease of artists that provided a painless death. Abdominal TB most commonly involves the ileocecal region and presents with abdominal pain, weight loss, and fever in young adults. Diagnosis relies on suggestive investigations and meeting criteria like histological evidence of caseating granulomas. Radiology may show features of peritoneal or intestinal involvement.