DEFINITION
• Chronic granulomatousmulti-systemic infection mostly affect the
lung and caused by infection with complex of micro-organism
(Mycobacteria).
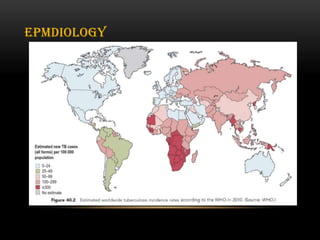
• Tuberculosis continues to be a major global health problem.
• The World Health Organization estimates that 2billion people (one-
third of the world’s population) have latent infection with
Mycobacterium tuberculosis, 8.6million people develop active
disease and 1.3million die each year from tuberculosis.
3.
• physicians inancient (Greece) called this illness as (phthisis)
reflecting it's wasting character.
• The classical and most common example of chronic infection of
the lungs.
4.
• M. tuberculosis
•M. bovis
• M. africanum
• M. microti
• M. canettii
• M. caprae
• M. pinnipedii
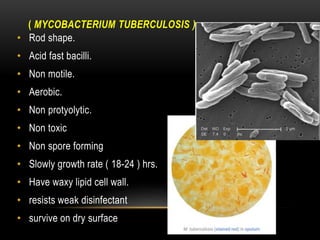
ETIOLOGY
( MYCOBACTERIUM TUBERCULOSIS)
• Rod shape.
• Acid fast bacilli.
• Non motile.
• Aerobic.
• Non protyolytic.
• Non toxic
• Non spore forming
• Slowly growth rate ( 18-24 ) hrs.
• Have waxy lipid cell wall.
• resists weak disinfectant
• survive on dry surface
7.
• Infectious dose:less than 10 bacilli.
• TB highly contiguous in active stage.
• Third of population in the world infected by latent TB.
Myco = mold like ( on the surface of liquid media, the growth
appears mold-like)
Tubercle = lump, knob ( isolated of microbe in a wall-off lesion
called (tubercle)
8.
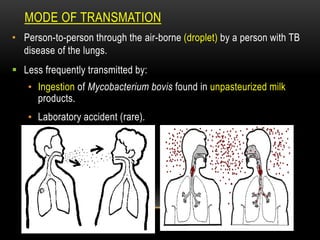
TRANSMATION
MODE OF
• Person-to-personthrough the air-borne (droplet) by a person with TB
disease of the lungs.
Less frequently transmitted by:
• Ingestion of Mycobacterium bovis found in unpasteurized milk
products.
• Laboratory accident (rare).
9.
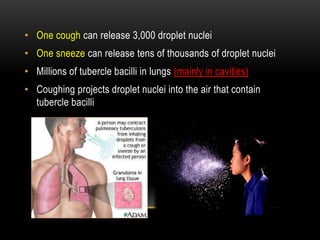
• One coughcan release 3,000 droplet nuclei
• One sneeze can release tens of thousands of droplet nuclei
• Millions of tubercle bacilli in lungs (mainly in cavities)
• Coughing projects droplet nuclei into the air that contain
tubercle bacilli
10.
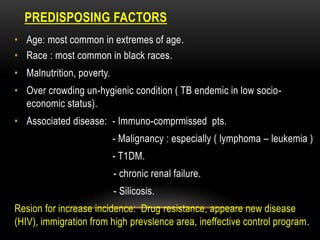
PREDISPOSING FACTORS
• Age:most common in extremes of age.
• Race : most common in black races.
• Malnutrition, poverty.
• Over crowding un-hygienic condition ( TB endemic in low socio-
economic status).
• Associated disease: - Immuno-comprmissed pts.
- Malignancy : especially ( lymphoma – leukemia )
- T1DM.
- chronic renal failure.
- Silicosis.
Resion for increase incidence: Drug resistance, appeare new disease
(HIV), immigration from high prevslence area, ineffective control program.
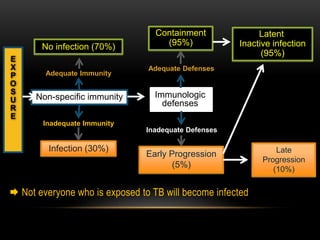
Not everyonewho is exposed to TB will become infected
No infection (70%)
Adequate Immunity
Non-specific immunity
Inadequate Immunity
Infection (30%)
E
X
P
O
S
U
R
E
Immunologic
defenses
Inadequate Defenses
Early Progression
(5%)
Adequate Defenses
Containment
(95%)
Late
Progression
(10%)
Latent
Inactive infection
(95%)
13.
DISEASE DIVIDED INTOTWO MAIN PATTERNS, PRIMARY
AND POST-PRIMARY ( SECONDARY TB ).
• Primary tuberculosis (TB childhood):
is the pattern of disease seen with first infection in a patient (often
a child) without specific immunity to tuberculosis.
• Infection is acquired by inhalation of organisms from an infected
individual, and the initial lesion typically develops in the
peripheral sub-pleural region of the lung.
14.
PRIMARY TB
• Theinitial infection with M. tuberculosis is known as primary
tuberculosis and usually occurs in the upper region of the lung
producing a subpleural lesion called the Ghon focus. The primary lesion
may also occur in the gastrointestinal tract, particularly the ileo-caecal
region. The primary focus is characterized by exudation and infiltration
with neutrophil granulocytes. These are replaced by macrophages
which engulf the bacilli and result in the typical granulomatous lesions,
which consist of central areas of caseation surrounded by epithelioid
cells and Langhans’ giant cells (both derived from the macrophage).
15.
• The primaryfocus is almost always accompanied by caseous
lesions in the regional lymph nodes (mediastinal and cervical) –
together these constitute the Ghon complex. In most people the
primary infection and the lymph nodes heal completely and
become calcified.
16.
• TB bacillican be avoid mucus traps ( physical barrier) and pass
to deep air way in alveoli..
• The macrophage in the alveoli can not lysis the bacteria after
phagocytic it ,due to waxy cell wall also organism can inhibit the
fusion between the phagosome and lysosome, inside the
macrophage
• hence the organism survive and replicate..
17.
• After afew weeks, disease symptoms appear as many of the
macrophages die, releasing tubercle bacilli and forming a caseous center
in the tubercle.
• The aerobic tubercle bacilli do not grow well in this location. However
many remain dormant (latent TB) and serve as a basis for later reactivation
of the disease. The disease may be arrested at this stage, and the lesions
become calcified.
• the LPS (lipopolysaccharide ) in the bacterial cell wall induce
macrophage to secrete TNF alpha which response for many symptoms
of TB: low grade fever - weight loss - night sweating...
• organism contain heat shock protein that stimulates T-lymphocyte
autoimmine reaction which causes further tissue damage.
18.
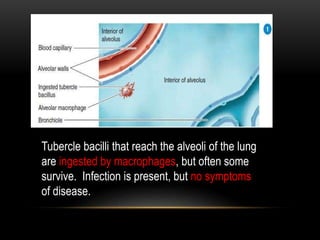
Tubercle bacilli thatreach the alveoli of the lung
are ingested by macrophages, but often some
survive. Infection is present, but no symptoms
of disease.
19.
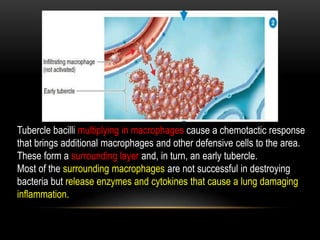
Tubercle bacilli multiplyingin macrophages cause a chemotactic response
that brings additional macrophages and other defensive cells to the area.
These form a surrounding layer and, in turn, an early tubercle.
Most of the surrounding macrophages are not successful in destroying
bacteria but release enzymes and cytokines that cause a lung damaging
inflammation.
20.
After a fewweeks, disease symptoms appear as many of the macrophages
die, releasing tubercle bacilli and forming a caseous center in the tubercle.
The aerobic tubercle bacilli do not grow well in this location. However,
many remain dormant (latent TB) and serve as a basis for later reactivation
of the disease. The disease may be arrested at this stage, and the lesions
become calcified.
21.
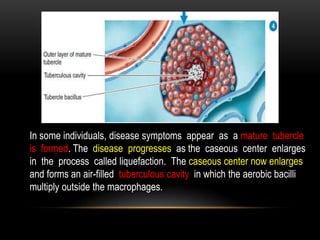
In some individuals,disease symptoms appear as a mature tubercle
is formed. The disease progresses as the caseous center enlarges
in the process called liquefaction. The caseous center now enlarges
and forms an air-filled tuberculous cavity in which the aerobic bacilli
multiply outside the macrophages.
22.
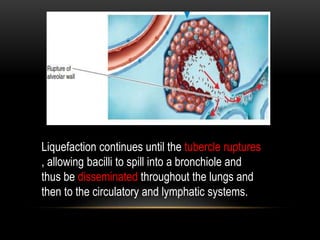
Liquefaction continues untilthe tubercle ruptures
, allowing bacilli to spill into a bronchiole and
thus be disseminated throughout the lungs and
then to the circulatory and lymphatic systems.
23.
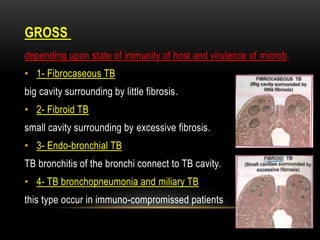
GROSS
depending upon stateof immunity of host and virulence of microb.
• 1- Fibrocaseous TB
big cavity surrounding by little fibrosis.
• 2- Fibroid TB
small cavity surrounding by excessive fibrosis.
• 3- Endo-bronchial TB
TB bronchitis of the bronchi connect to TB cavity.
• 4- TB bronchopneumonia and miliary TB
this type occur in immuno-compromissed patients
24.
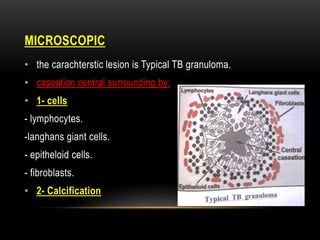
MICROSCOPIC
• the carachtersticlesion is Typical TB granuloma.
• caseation central surrounding by:
• 1- cells
- lymphocytes.
-langhans giant cells.
- epitheloid cells.
- fibroblasts.
• 2- Calcification
25.
TUBERCULOSIS
CLINICAL FEATURES OFPRIMARY
• I. Symptoms and signs of infection, i.e. fever, influenza like illness ,
primary complex, skin test conversion.
• II. Symptoms and signs of the disease, i.e. lymphadenopathy (hilar,
paratracheal, mediastinal), collapse or consolidation (right middle
lobe), obstructive emphysema, pleural effusion, endo-bronchial
tuberculosis, miliary tuberculosis or, meningitis and pericarditis.
• III. Symptoms and signs of hypersensitivity, e.g. erythema nodosum,
phylectenular conjunctivitis, dactylitis.
26.
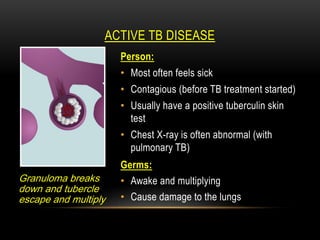
ACTIVE TB DISEASE
Granulomabreaks
down and tubercle
escape and multiply
Person:
• Most often feels sick
• Contagious (before TB treatment started)
• Usually have a positive tuberculin skin
test
• Chest X-ray is often abnormal (with
pulmonary TB)
Germs:
• Awake and multiplying
• Cause damage to the lungs
27.
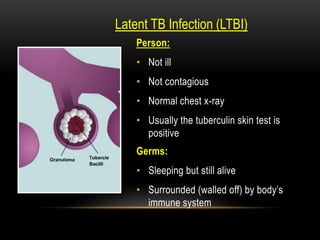
Latent TB Infection(LTBI)
Person:
• Not ill
• Not contagious
• Normal chest x-ray
• Usually the tuberculin skin test is
positive
Germs:
• Sleeping but still alive
• Surrounded (walled off) by body’s
immune system
29.
MANIFESTATIONS
OF MAJOR
CLINICAL PRESENTATIONS
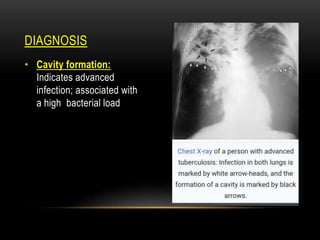
•1. cavity
• 2. Consolidation or collapse
• 3. Pleural effusion/empyema
• 4. Miliary tuberculosis
• 5. Hydropneumothorax or branchopleural fistula
• 6. Hilar lymphadenopathy
• 7. Bronchiectasis.
30.
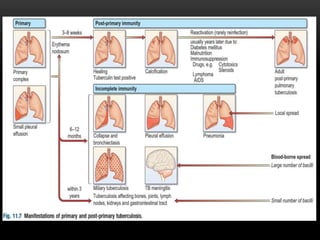
THE FATE OFTHE PRIMARY COMPLEX IS AS FOLLOWS:
• 1. It may heal spontaneously within 1-2 months and tuberculin skin
test becomes positive.
• 2. Spread of the primary focus to hilar and mediastinal lymph nodes
to form primary complex which in most cases heals spontaneously.
• 3. It may remain dormant, becomes reactivated when the body
defenses are lowered.
• 4. Direct extension of primary focus – called progressive pulmonary
tuberculosis merging with post-primary TB.
• 5. Hematogenous spread leading to miliary tuberculosis, or
tubercular meningitis.
31.
OF TB
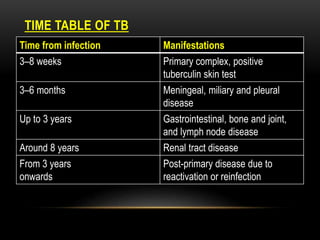
TIME TABLE
Manifestations
Timefrom infection
Primary complex, positive
tuberculin skin test
3–8 weeks
Meningeal, miliary and pleural
disease
3–6 months
Gastrointestinal, bone and joint,
and lymph node disease
Up to 3 years
Renal tract disease
Around 8 years
Post-primary disease due to
reactivation or reinfection
From 3 years
onwards
32.
TB
MILIARY
• Blood-borne disseminationgives rise to miliary TB, which may present
acutely but more frequently is characterised by 2–3 weeks of fever,
night sweats, anorexia, weight loss and a dry cough.
• Hepatomegaly may developed and the spleen may be palpable.
• The presence of a headache may indicate coexistent tuberculous
meningitis.
• Auscultation of the chest is frequently normal, although with more
advanced disease widespread crackles are evident.
• Fundoscopy may show choroidal tubercles.
33.
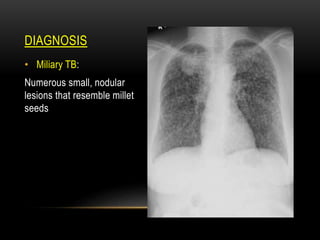
MILIARY TB
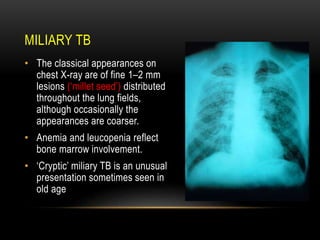
• Theclassical appearances on
chest X-ray are of fine 1–2 mm
lesions (‘millet seed’) distributed
throughout the lung fields,
although occasionally the
appearances are coarser.
• Anemia and leucopenia reflect
bone marrow involvement.
• ‘Cryptic’ miliary TB is an unusual
presentation sometimes seen in
old age
34.
CRYPTIC TUBERCULOSIS
• ‘cryptic’means ‘hidden’ ,patient of tuberculosis with normal chest radiog
raph is called cryptic tuberculosis.
Its presentation is as follows:
• Age over 60 years
• Intermittent low grade fever (PUO) with night sweats and evening rise
• Unexplained weight loss, general debility
• Hepatosplenomegaly (seen in 25% cases only) • Normal chest X-ray
• Negative tuberculin skin test
• Leukaemoid reaction or pancytopenia
• Confirmation is done by biopsy (liver or bone marrow).
35.
SECONDARY TB
• Mostcommonly clinical tuberculosis represents delayed reactivation.
this term used to describe lung disease, Post-primary disease refers to
exogenous (‘new’ infection) or endogenous (reactivation of a dormant
primary lesion) infection in a person who has been sensitised by earlier
exposure.
• The onset is usually insidious, developing slowly over several weeks.
• It is most frequently pulmonary and characteristically occurs in the
apex of an upper lobe where the oxygen tension favours survival of
the strictly aerobic organism.
• Systemic symptoms include fever, night sweats, malaise, and loss of
appetite
36.
• tuberculus cavity,or granuloma discharged into the bronchus.
• massive pulmonary involvement, and may be produces
(tuberculus pneumonia)
• common site: localized in one or both upper lobes, superior
segments of lower lobes usually involved due to high oxygen
concentration. that favors mycobacterium growth.
37.
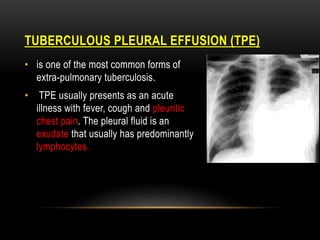
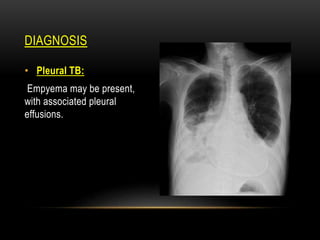
PLEURAL EFFUSION (TPE)
TUBERCULOUS
•is one of the most common forms of
extra-pulmonary tuberculosis.
• TPE usually presents as an acute
illness with fever, cough and pleuritic
chest pain. The pleural fluid is an
exudate that usually has predominantly
lymphocytes.
38.
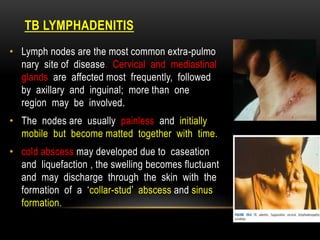
TB LYMPHADENITIS
• Lymphnodes are the most common extra-pulmo
nary site of disease. Cervical and mediastinal
glands are affected most frequently, followed
by axillary and inguinal; more than one
region may be involved.
• The nodes are usually painless and initially
mobile but become matted together with time.
• cold abscess may developed due to caseation
and liquefaction , the swelling becomes fluctuant
and may discharge through the skin with the
formation of a ‘collar-stud’ abscess and sinus
formation.
DISEASE
GASTROINTESTINAL
• Upper gastrointestinaltract involvement is rare and is usually an
unexpected histological finding in an endoscopic or laparotomy
specimen.
• swallowing of the infected sputum , hematological spread or ingestion
of cow milk which infected with bovine strain are important
pathological mechanisms of GIT involved.
• terminal ileum and cecum are most common involved.
• abdominal pain, chronic diarrhea, malabsorption and intestinal
obstruction and right iliac fossa mass may be palpable.
Up to 30% of cases present with an acute abdomen. Ultrasound or
CT may reveal thickened bowel wall, abdominal lymphadenopathy,
mesenteric thickening or ascites.
41.
• The maindifferential diagnosis is Crohn’s disease.
• Tuberculous peritonitis may developed from direct spread of
lymphatic ruptured or by hematogenous spread.
• lymph nodes is characterized by abdominal distension, pain
and constitutional symptoms. The ascitic fluid is exudative
and cellular with a predominance of lymphocytes.
• Low-grade hepatic dysfunction is common in miliary disease
when biopsy reveals granulomas.
42.
PERICARDIAL DISEASE
• Diseaseoccurs in two forms:
Pericardial effusion
constrictive pericarditis
• Constrictive pericarditis with thick pericardium
,calcification and fibrosis is main complication.
• Effusion is exudate and may be hemorrhage.
• The addition of corticosteroids to anti-
tuberculosis treatment has been shown to
be beneficial for both forms of pericardial
disease.
43.
MENINGEAL DISEASE
• Centralnervous system disease Meningeal disease represents
the most important form of central nervous system TB
• ocular nerve palsy is common, and hydrocephalus is the main
complication.
• corticosteroid therapy is essential under umbrella of antibiotic
for prevent hydrocephalus formation.
• untreated, it is rapidly fatal.
44.
DISEASE
BONE AND JOINT
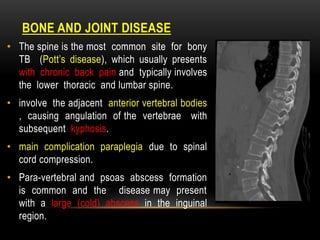
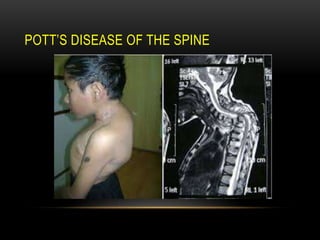
•The spine is the most common site for bony
TB (Pott’s disease), which usually presents
with chronic back pain and typically involves
the lower thoracic and lumbar spine.
• involve the adjacent anterior vertebral bodies
, causing angulation of the vertebrae with
subsequent kyphosis.
• main complication paraplegia due to spinal
cord compression.
• Para-vertebral and psoas abscess formation
is common and the disease may present
with a large (cold) abscess in the inguinal
region.
• TB canaffect any joint, but most frequently involves the
hip or knee.
• tuberculus of hip joint cause pain and limping , while tuberculus
of knee cause pain and swelling of joint.
• if progressive reduction in joint space and erosions appear.
47.
DISEASE
GENITOURINARY
• Fever andnight sweats are rare with renal tract TB and
patients are often only mildly symptomatic for many years
• hematuria , dysuria, increase frequency of maturation and flank
pain may be the symptoms.
• Patient may present first with complication:
- sterile pyuria ( pus cells but no bacteria in the urine).
- In women, infertility from endometritis, or pelvic pain and swelling
from salpingitis or a tubo- ovarian abscess occur occasionally.
- In men, genitourinary TB may present as epididymitis or prostatitis.
49.
SYMPTOMS
Classic clinicalfeatures associated with active pulmonary TB are as
follows (elderly individuals with TB may not display typical signs and
symptoms):
• Cough
• Weight loss/anorexia
• Fever
• Night sweats
• Hemoptysis
• Chest pain (can also result from tuberculous acute pericarditis)
• Fatigue
50.
SYMPTOMS
Symptoms oftuberculous meningitis may include the following:
• Headache that has been either intermittent or persistent for 2-3
weeks.
• Subtle mental status changes that may progress to coma over
a period of days to weeks.
• Low-grade or absent fever.
51.
SYMPTOMS
Symptoms ofskeletal TB may include the following:
• Back pain or stiffness.
• Lower-extremity paralysis, in as many as half of patients with
undiagnosed Pott’s disease.
• Tuberculous arthritis, usually involving only 1 joint (most often
the hip or knee, followed by the ankle, elbow, wrist, and
shoulder)
52.
SYMPTOMS
Symptoms ofgenitourinary TB may include the following:
• Flank pain
• Dysuria
• Frequent urination
• In men, a painful scrotal mass, prostatitis, orchitis, or epididymitis
• In women, symptoms mimicking pelvic inflammatory disease
53.
SYMPTOMS
Symptoms ofgastrointestinal TB are referable to the infected
site and may include the following:
• Non-healing ulcers of the mouth or anus.
• Difficulty swallowing (with esophageal disease).
• Abdominal pain mimicking peptic ulcer disease (with gastric or
duodenal infection).
• Mal-absorption (with infection of the small intestine).
• Pain, diarrhea, or hematochezia (with infection of the colon)
54.
PHYSICAL EXAMINATION
Physicalexamination findings associated with TB depend on the
organs involved. Patients with pulmonary TB may have the
following:
• Right iliac fossa mass.
• Abnormal breath sounds, especially over the upper lobes or
involved areas
• Rales or bronchial breath signs, indicating lung consolidation
55.
PHYSICAL EXAMINATION
Signsof extra-pulmonary TB differ according to the tissues
involved and may include the following:
• Confusion.
• Coma.
• Neurologic deficit.
• Lymphadenopathy.
• Cutaneous lesions.
56.
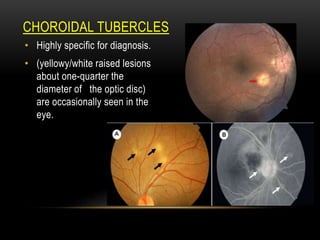
TUBERCLES
CHOROIDAL
• Highly specificfor diagnosis.
• (yellowy/white raised lesions
about one-quarter the
diameter of the optic disc)
are occasionally seen in the
eye.
57.
PHYSICAL EXAMINATION
• Theabsence of any significant physical findings does not
exclude active TB.
• Classic symptoms are often absent in high-risk patients,
particularly those who are immuno-compromised or elderly.
58.
CHRONIC COMPLICATION OFPULMONARY TUBERCULOSIS
1. Pulmonary complications
• pleurisy
with or without pleural effusion, Lung/pleural calcification
• pneumothorax
may follow rupture of tuberculous lesion into the pleural space.
• empyema or pyopneumothorax
serious complication of rupture of tuberculous lesion into the pleura
l space.
59.
• fungal colonizationof cavity
cavity which persist after anti-TB treatment may be colonized with
aspergillus fumigatus and a ball of fungus may develop.
• Massive hemoptysis.
• Bronchiectasis
• Broncho-pleural fistula
60.
2. Non-pulmonary complications
•tuberculous laryngitis
usually only occur in advanced pulmonary disease
• tuberculous enteritis
follows swallowing heavily infected sputum in some patient with exc
essive pulmonary disease
• Ischiorectal abscess
consider TB in all cases, Tubercle bacilli can pass through rectal mu
cosa.
61.
• blood bornedissemination
uncommon complication of post primary pulmonary disease ,except
in immuno-comprmissed patients.
• Respiratory failure and right ventricular failure
late complication when disease has caused extensive pulmonary di
struction and fibrosis.
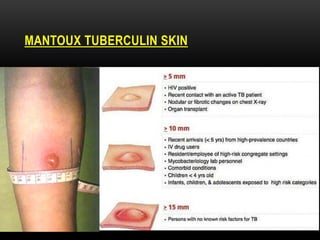
DIAGNOSIS
Screening methodsfor TB include the following:
• Mantoux tuberculin skin .
• chest radiograph to evaluate for possible associated pulmonary
findings.
• In vitro blood test based on interferon gamma release assay
(IGRA)
• Acid-fast bacilli (AFB) smear and culture.
• HIV serology in all patients with TB and unknown HIV status.
64.
DIAGNOSIS
• Mantoux tuberculinskin test with purified protein derivative
(PPD) for active or latent infection (primary method).
MICROSCOPIC
• 3 consecutivemorning specimens in 3 consecutive days.
• - specimens should by obtained from lung secretions not saliva.
• - If sputum not avalible :
• laryngeal swab or trans-tracheal aspiration.
67.
DIAGNOSIS
• chest radiograph:
Obtain a chest radiograph to evaluate for possible associated
pulmonary findings. The following patterns may be seen:
• Noncalcified round infiltrates: May be confused with lung carcinoma
• Homogeneously calcified nodules (usually 5-20 mm):Tuberculomas
, representing old infection.
• Primary TB: Typically, pneumonia like picture of infiltrative process
in middle or lower lung regions.
DIAGNOSIS
• Reactivation TB:Pulmonary lesions in posterior segment of right
upper lobe, apico-posterior segment of left upper lobe, and apic
al segments of lower lobes.
• TB associated with HIV disease: Frequently atypical lesions or
normal chest radiographic findings.
• Healed and latent TB: Dense pulmonary nodules in hilar or
upper lobes; smaller nodules in upper lobes.
.
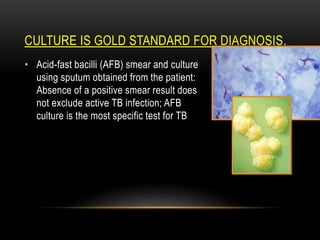
CULTURE IS GOLDSTANDARD FOR DIAGNOSIS
• Acid-fast bacilli (AFB) smear and culture
using sputum obtained from the patient:
Absence of a positive smear result does
not exclude active TB infection; AFB
culture is the most specific test for TB
74.
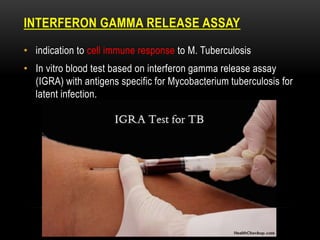
INTERFERON GAMMA RELEASEASSAY
• indication to cell immune response to M. Tuberculosis
• In vitro blood test based on interferon gamma release assay
(IGRA) with antigens specific for Mycobacterium tuberculosis for
latent infection.
DIAGNOSIS
• Obtain thefollowing laboratory tests for patients with suspected
TB:
HIV serology in all patients with TB and unknown HIV status:
Individuals infected with HIV are at increased risk for TB.
77.
DIAGNOSIS
Other diagnostictesting may warrant consideration, including
the following:
• Specific enzyme-linked immunospot (ELISpot)
• Nucleic acid amplification tests
• Blood culture
78.
DIAGNOSIS
Workup considerationsfor extra-pulmonary TB include the
following:
• Biopsy of bone marrow, liver, or blood cultures
• If tuberculous meningitis or tuberculoma is suspected, perform
lumbar puncture
• If vertebral (Pott’s disease) or brain involvement is suspected,
CT or MRI is necessary
• If genitourinary complaints are reported, urinalysis and urine
cultures can be obtained
80.
MANAGEMENT
Physical measures(if possible or practical) include the
following:
• Isolate patients with possible TB in a private room with negative
pressure.
• Have medical staff wear high-efficiency disposable masks
sufficient to filter the bacillus.
• Continue isolation until sputum smears are negative for 3
consecutive determinations (usually after approximately 2-4
weeks of treatment).
81.
MANAGEMENT
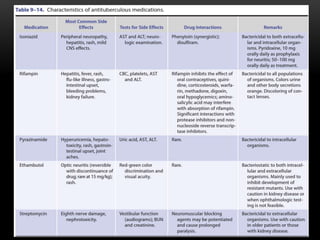
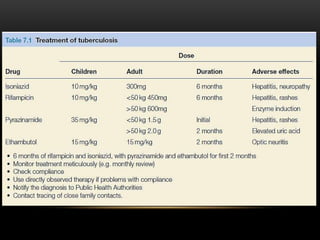
• Initial empiricpharmacologic therapy consists of the following
4-drug regimens:
• Isoniazid
• Rifampin
• Pyrazinamide
• Either ethambutol or streptomycin
84.
Prevention and chemoprophylaxis
Close contacts of a case are screened for evidence of disease with a
chest X-ray and a Mantoux test (positive if area of induration10 mm 72
hours after intradermal injection of purified protein derivative of
Mycobacterium TB) or whole blood interferon-γ assay.
Vaccination with BCG (bacille Calmette–Guerin) reduces the risk of
developing tuberculosis