Downloaded 2,941 times
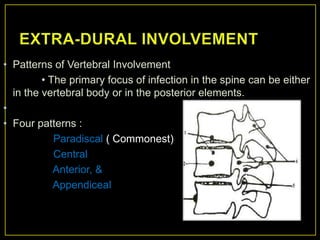
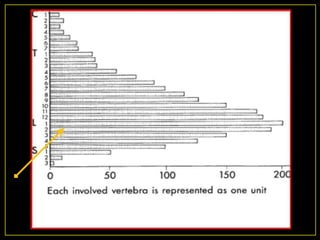
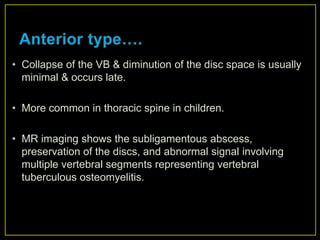

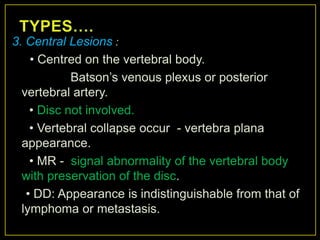

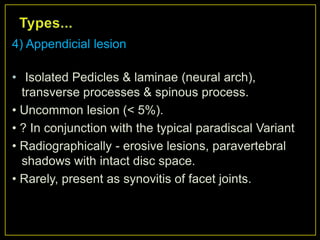
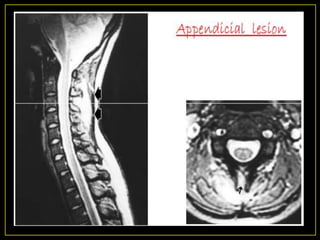
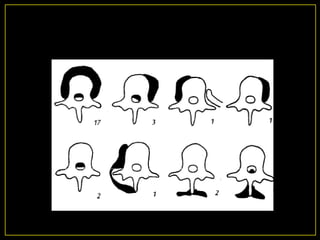
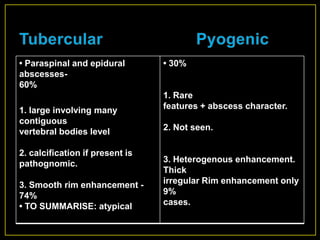
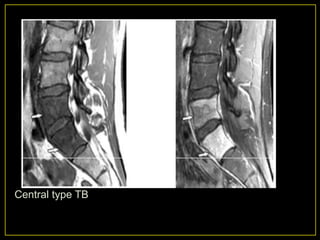


The document discusses spinal tuberculosis, noting that it causes delays in diagnosis, long recovery periods, and high costs. Key points include: - Paralysis occurs in up to 50% of spinal tuberculosis patients. - Early diagnosis, expedient treatment, aggressive surgery, and preventing deformity lead to the best outcomes. - Diagnosis relies on tests like tuberculin skin tests, imaging like MRI to identify bone destruction and abscesses, and microscopy and culture of samples. - Patterns of bone involvement include paradiscal, central, anterior, and appendiceal lesions. - Complications include paralysis, cold abscesses, deformities, and secondary infections.


















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















