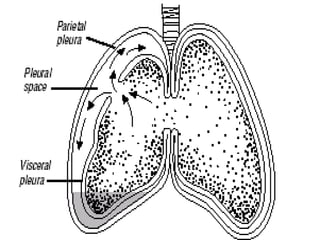
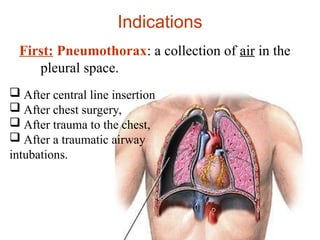
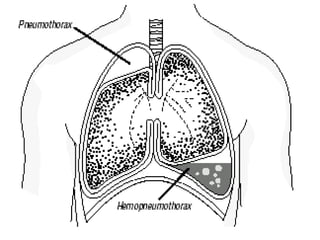
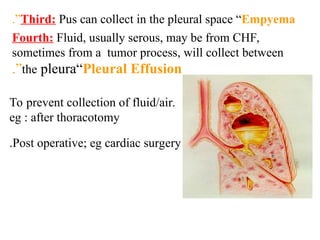
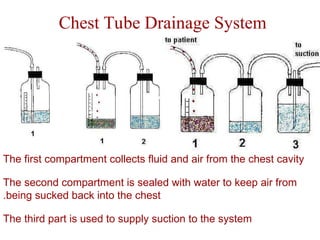
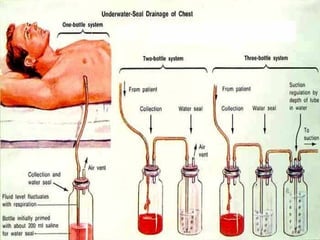
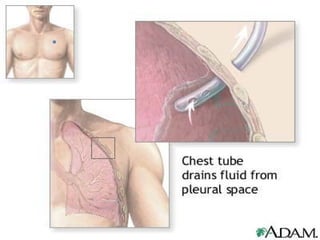
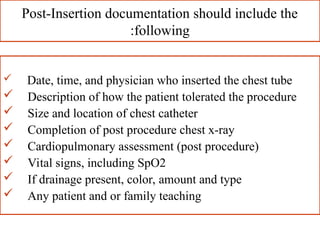
Chest tubes are used to evacuate air or fluid from the pleural or mediastinal space, especially in cases of pneumothorax, hemothorax, or pleural effusion, allowing the lung to re-expand. The insertion involves sterile techniques and appropriate equipment, and post-insertion care focuses on maintaining the system's patency and sterility to prevent complications like tension pneumothorax. Proper monitoring and assessment of the chest tube system are essential for patient outcomes such as lung re-expansion and infection prevention.




































































![Acute_respiratory_failure[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterespiratoryfailure1autosaved-240613055024-837043a9-thumbnail.jpg?width=640&height=640&fit=bounds)






















