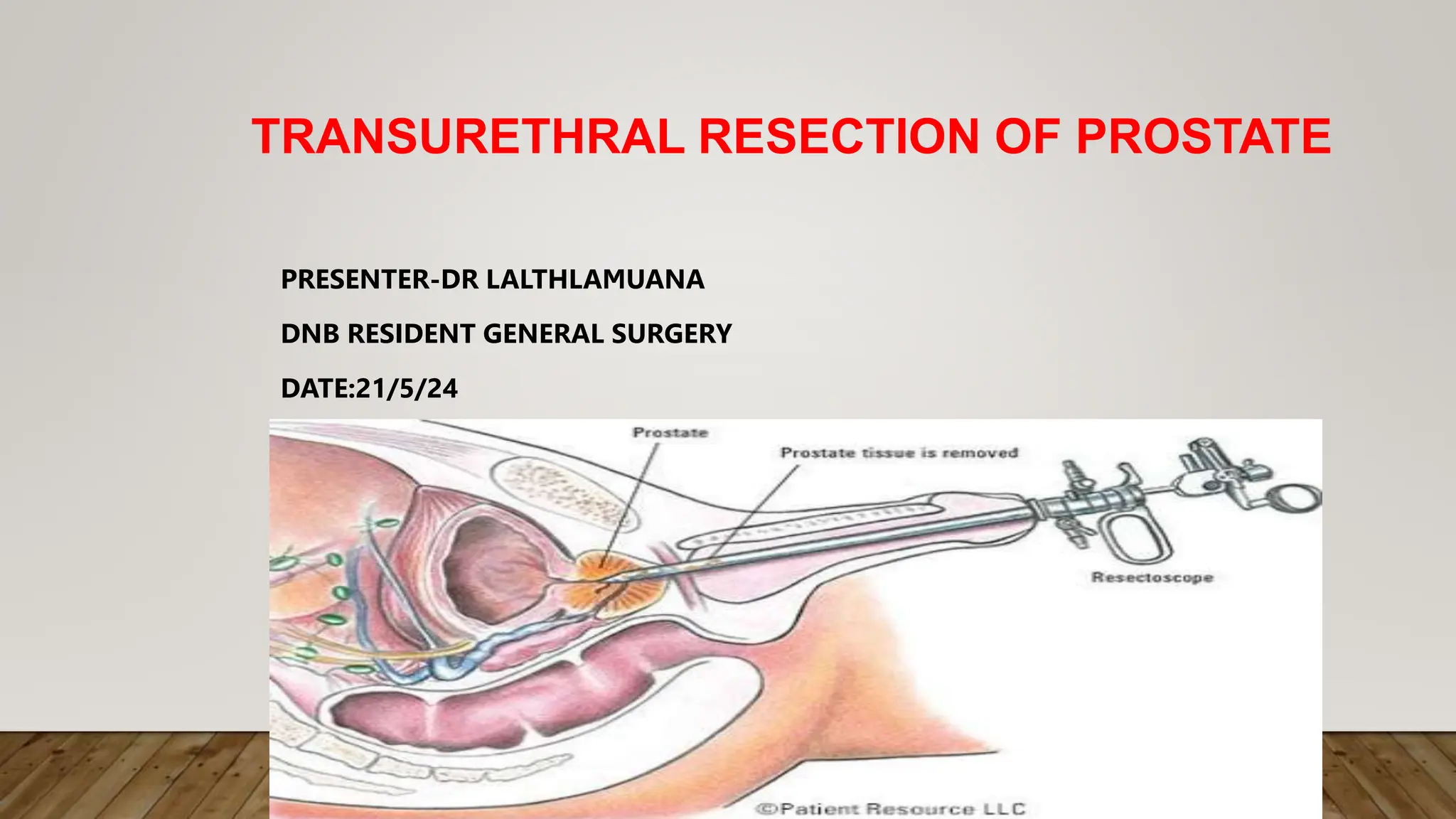
Transurethral resection of the prostate (TURP) is a surgical procedure to remove parts of the prostate gland through the urethra, primarily indicated for benign prostatic hyperplasia with symptoms. The surgery is performed using a resectoscope and typically lasts 30-60 minutes, with potential complications such as TURP syndrome due to excessive irrigation fluid absorption. Early recognition and prompt treatment of complications are crucial, as the procedure is commonly performed on elderly patients with coexisting diseases.
































































![A PROSPECTIVE STUDY COMPARING PERIOPERATIVE AND [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aprospectivestudycomparingperioperativeandautosaved-240222145726-4f79a098-thumbnail.jpg?width=640&height=640&fit=bounds)


























