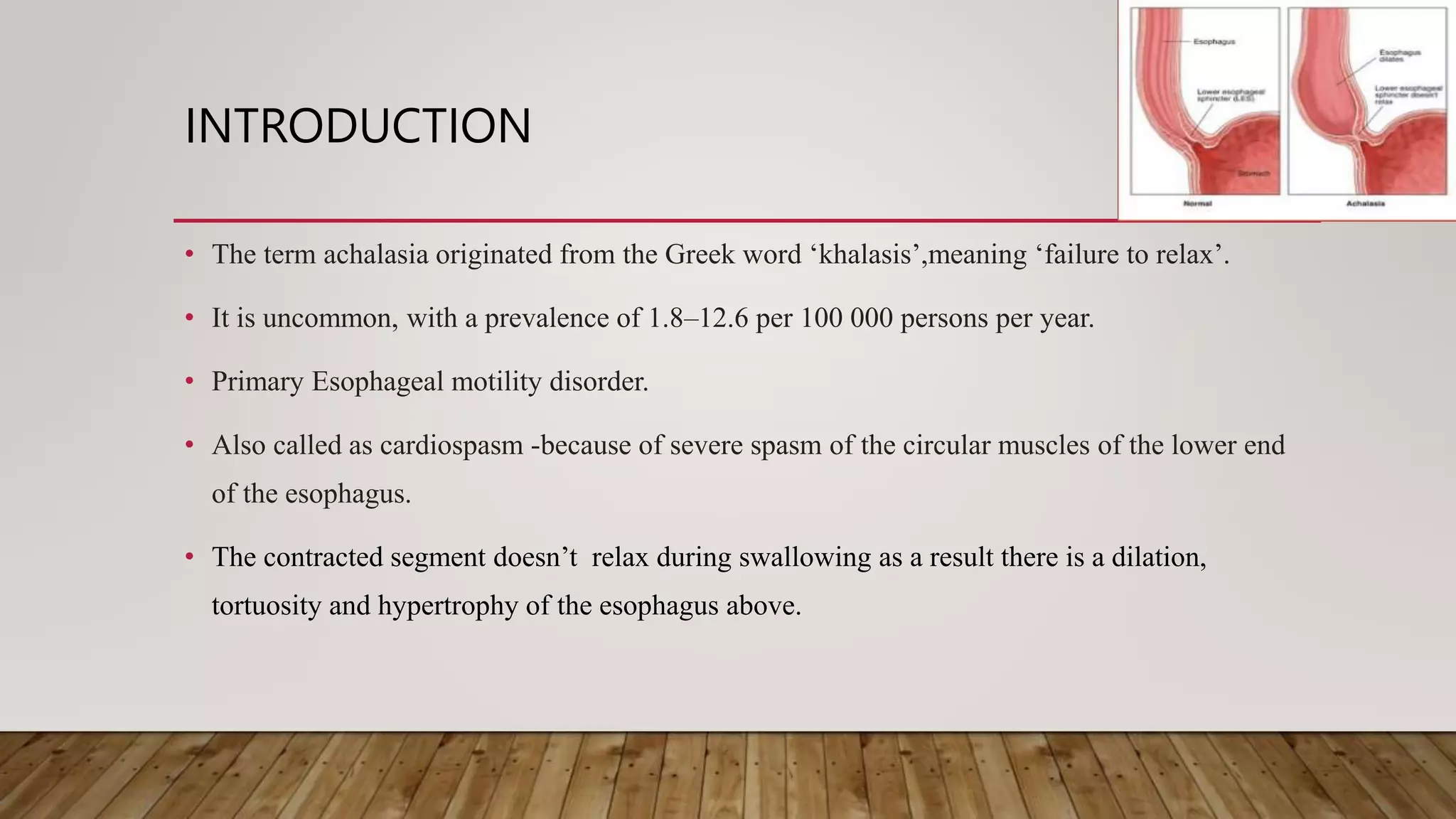
- Achalasia is a rare esophageal motility disorder caused by the loss of inhibitory ganglion cells in the esophagus. This results in failure of the lower esophageal sphincter to relax during swallowing.
- Symptoms include dysphagia, regurgitation, and chest pain. Over time the esophagus dilates and food can pool, leading to complications.
- Diagnosis involves endoscopy, barium swallow, and high-resolution manometry showing failure of the LES to relax. Treatment aims to reduce LES pressure and includes medications, botulinum toxin injection, pneumatic dilation, Heller's myotomy, and occasionally surgery. Newer treatments like peroral end























































































![A PROSPECTIVE STUDY COMPARING PERIOPERATIVE AND [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aprospectivestudycomparingperioperativeandautosaved-240222145726-4f79a098-thumbnail.jpg?width=640&height=640&fit=bounds)



















