1. The document discusses potential adverse effects of blood transfusions, including immediate effects like acute hemolytic transfusion reactions and delayed effects such as transmission of infections.
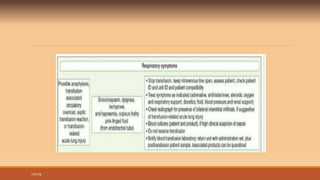
2. It provides guidance on recognizing and investigating transfusion reactions, stating that all post-transfusion reactions should initially be considered hemolytic. Steps include stopping the transfusion, checking paperwork for errors, and obtaining samples for testing.
3. Tests are described to detect evidence of hemolysis or blood group incompatibility, and to check for complications like disseminated intravascular coagulation or acute renal failure.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















