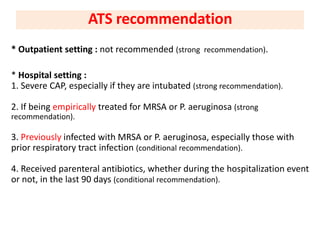
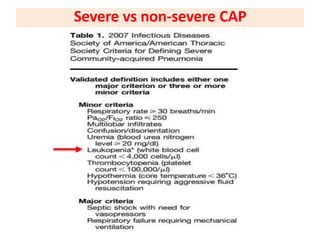
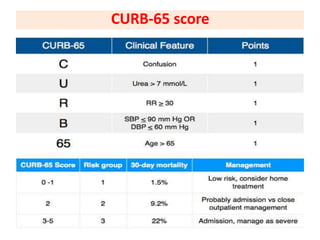
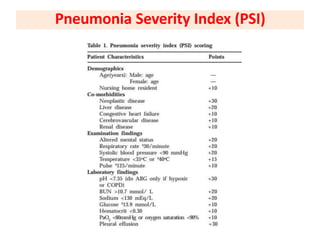
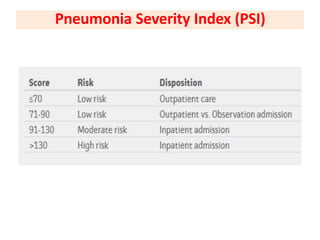
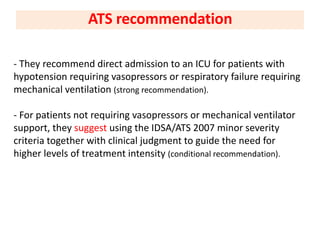
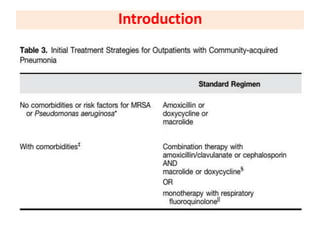
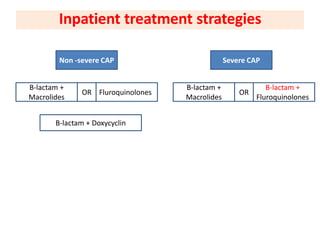
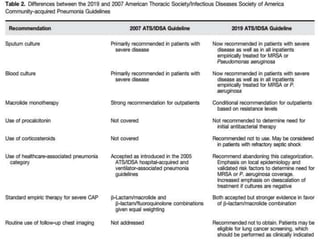


This document summarizes the recommendations from ATS guidelines for the diagnosis and treatment of community-acquired pneumonia in adults. It addresses 16 questions related to testing and treatment approaches. Key recommendations include only obtaining lower respiratory samples for severe CAP patients, using prediction rules like the Pneumonia Severity Index to determine hospitalization and ICU needs, and initial antibiotic treatment with beta-lactams plus macrolides or fluoroquinolones for non-severe CAP and beta-lactams plus fluoroquinolones or beta-lactams plus doxycycline for severe CAP. Antiviral therapy is recommended for influenza-positive patients along with standard antibacterial treatment.























































































