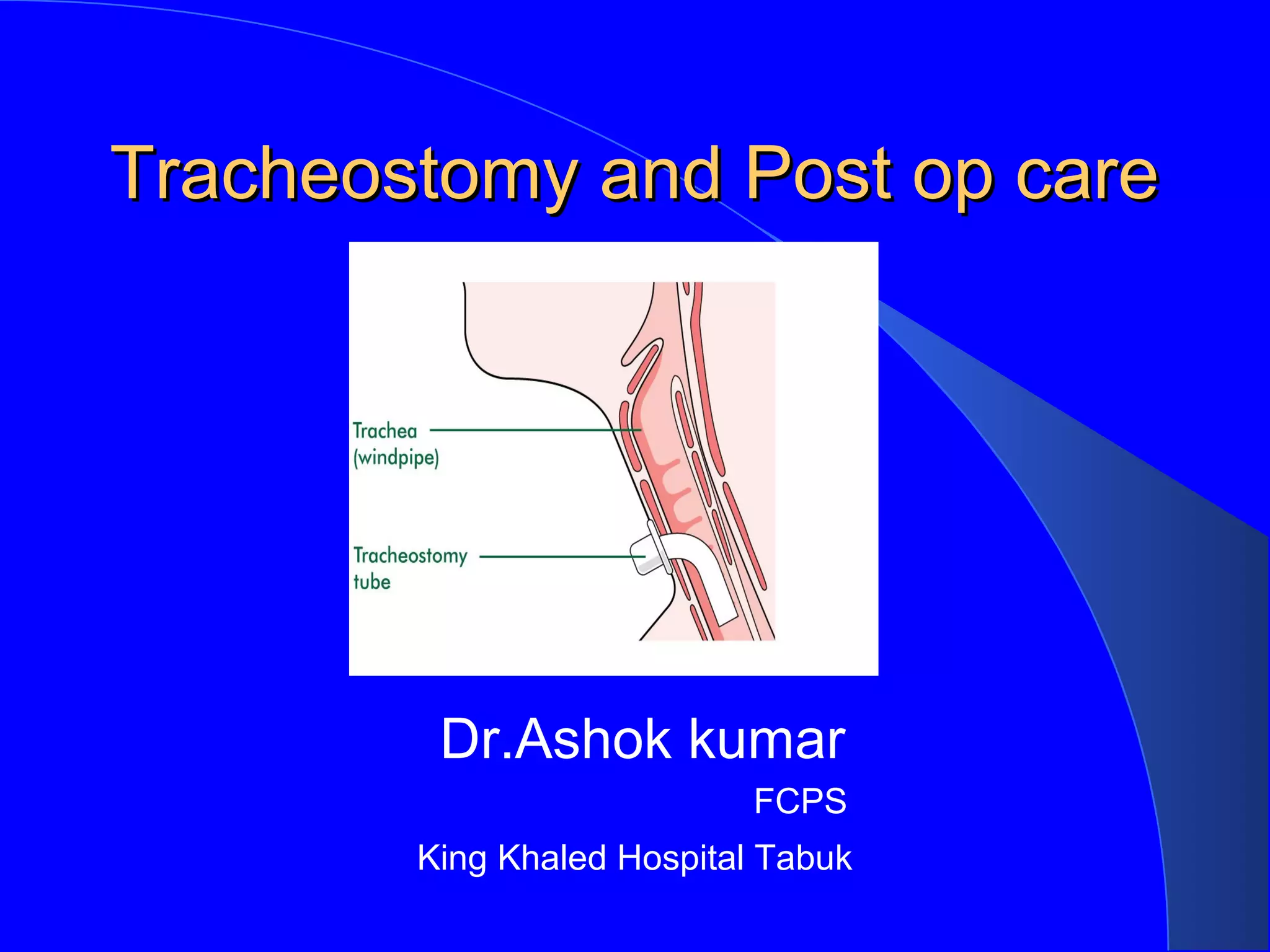
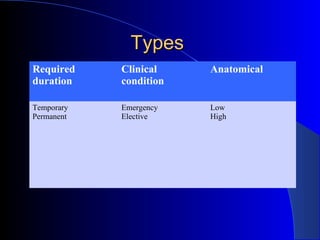
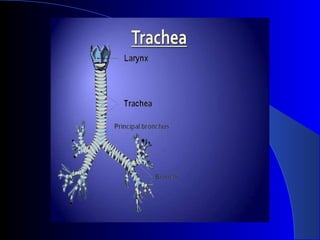
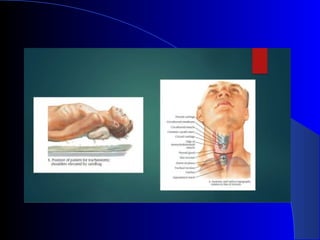
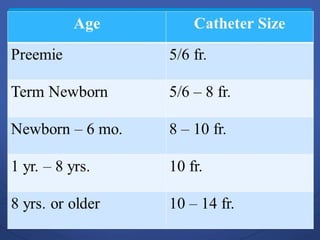
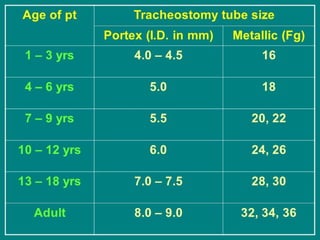
This document discusses tracheostomy and post-operative care. It defines tracheostomy as a surgical opening created in the anterior wall of the cervical trachea. It then covers the history of tracheostomy, indications for the procedure, operative technique, potential complications, prevention of complications, and post-operative care including education of the patient.