Medical Therapy
• Adjunctiverole
• Help to clear the cornea to facilitate angle surgery preoperatively
• postoperatively, they may help control IOP until the adequacy of the
surgical procedure has been verified.
3.
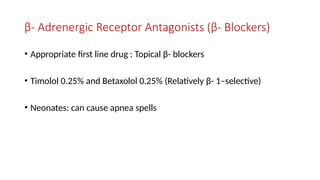
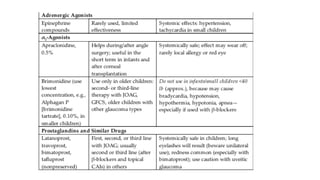
β- Adrenergic ReceptorAntagonists (β- Blockers)
• Appropriate first line drug : Topical β- blockers
• Timolol 0.25% and Betaxolol 0.25% (Relatively β- 1–selective)
• Neonates: can cause apnea spells
5.
Carbonic Anhydrase Inhibitors
•Reducing the IOP by about 20% to 35%.
• Orally with food or milk two, three, or four times daily(total daily dosage, 10–20
mg/kg).
• Topical CAI – Dorzolamide 2% and Brinzolamide 1%
- Although it is safer than full- dose oral acetazolamide, dorzolamide must
still be used with caution because there have been case reports of
neonates developing metabolic acidosis attributed to use of topical
dorzolamide
7.
• Miotics, whichparadoxically may increase the IOP by collapsing the
trabecular meshwork owing to the high insertion of uveal tissue into
the posterior meshwork.
9.
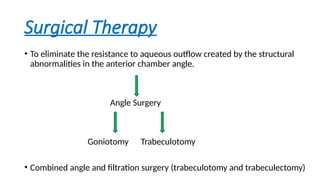
Surgical Therapy
• Toeliminate the resistance to aqueous outflow created by the structural
abnormalities in the anterior chamber angle.
Angle Surgery
Goniotomy Trabeculotomy
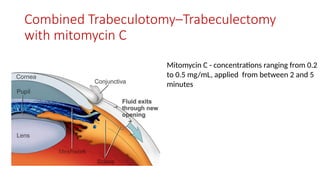
• Combined angle and filtration surgery (trabeculotomy and trabeculectomy)
10.
Goniotomy
• Otto Barkanintroduced the technique for PCG in 1938.
• Greek gonio - “angle,” and tomein - “to cut”
• Open a route for aqueous humor to exit the anterior chamber into the
Schlemm canal by removing obstructing tissue.
• Greatest success - PCG presenting between 3 and 12 months of age(80% to
more than 90%).
• PCG presenting at birth or after 12 months of age –success rate is about 30%–
50%.
11.
Technique
• Using asurgical goniolens (Barkan goniolens, including the Lister
modification, Swan–Jacobs lens, Hill goniolens and Khaw surgical
goniolens) and a goniotomy knife or needle.
• Effective TM incision: Make incision superficial and into anterior TM,
passing first one direction, then the other.
12.
• Surgeon usuallysits opposite to the portion of the angle to be operated (i.e., to the temporal
side of the patient for nasal goniotomy), with the patient’s head slightly rotated away from the
surgeon.
• Goniolens is placed over the cornea.
• The goniotomy knife or needle enters the anterior chamber through peripheral clear cornea 1
mm from the limbus, opposite to the midpoint of the intended goniotomy.
• The knife or needle is guided over iris tissue to engage trabecular meshwork in its anterior third,
just posterior to the Schwalbe line.
• A circumferential incision is then made for about 4 to 5 clock- hours. The incision should be
superficial.
• A deeper cleft with exposure of whiter tissue may be noted in the wake of the incision, with a
widening of the angle, and a posterior movement of peripheral iris in some cases.
13.
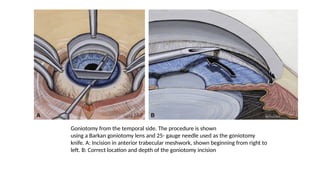
Goniotomy from thetemporal side. The procedure is shown
using a Barkan goniotomy lens and 25- gauge needle used as the goniotomy
knife. A: Incision in anterior trabecular meshwork, shown beginning from right to
left. B: Correct location and depth of the goniotomy incision
14.
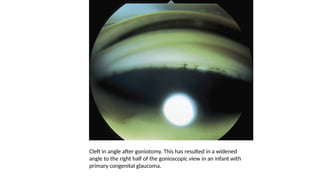
Cleft in angleafter goniotomy. This has resulted in a widened
angle to the right half of the gonioscopic view in an infant with
primary congenital glaucoma.
Trabeculotomy Ab Externo
•Cannulating the Schlemm canal from an external approach and then
tearing through the trabecular meshwork into the anterior chamber,
creates a direct communication between the anterior chamber and
Schlemm canal.
• Success rates varying from 73% to 100% in PCG
• Not limited by an edematous or scarred cornea.
17.
Technique
• Conjunctival flapand a partial- thickness triangular or rectangular
scleral flap are created.
• A radial scratch incision is made in the bed of the scleral flap
across the sclero limbal junction- gradually deepened until the Schlemm canal is
identified just anterior to the circumferential fibers of the scleral spur (near the
posterior aspect of the limbal “gray zone”). Often, a small amount of blood or
aqueous humor refluxes through the cut ends of the Schlemm canal, and the
internal wall of the canal appears slightly pigmented.
18.
• Anterior chamberentry and air bubble injected.
• Internal arm of a trabeculotome should be passed gently into the
canal (to the right side first for a right- handed surgeon) as far as
possible without meeting excessive resistance and by using the
parallel external arm as a guide.
• Rotation of the trabeculotome into the anterior chamber tears
through the intervening trabecular meshwork and requires little force.
• Haulted once about 75% to 80% of the internal arm of the
trabeculotome is visible in the anterior chamber.
19.
• In similarfashion, the trabeculotome should be placed into the left
side.
• scleral flap is then sutured
20.
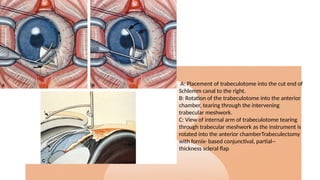
A: Placement oftrabeculotome into the cut end of
Schlemm canal to the right.
B: Rotation of the trabeculotome into the anterior
chamber, tearing through the intervening
trabecular meshwork.
C: View of internal arm of trabeculotome tearing
through trabecular meshwork as the instrument is
rotated into the anterior chamberTrabeculectomy
with fornix- based conjunctival, partial--
thickness scleral flap
21.
Complications
• Hyphema
• Inadvertentfiltering blebs
• Choroidal detachment
• Iridotomy
• Damage to the lens
• Creation of a false passage into the anterior chamber or suprachoroidal
space
• Infection
22.
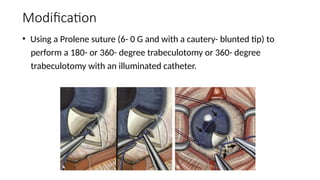
Modification
• Using aProlene suture (6- 0 G and with a cautery- blunted tip) to
perform a 180- or 360- degree trabeculotomy or 360- degree
trabeculotomy with an illuminated catheter.
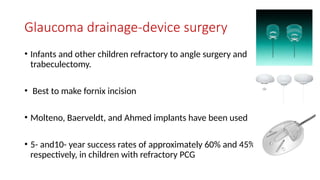
Glaucoma drainage-device surgery
•Infants and other children refractory to angle surgery and
trabeculectomy.
• Best to make fornix incision
• Molteno, Baerveldt, and Ahmed implants have been used
• 5- and10- year success rates of approximately 60% and 45%,
respectively, in children with refractory PCG
25.
Cyclodestructive procedures
• success- about 50%)
• Results are often unpredictable
• Complications are high
• Cyclocryotherapy and Transscleral cyclophotocoagulation with the
contact Nd:YAG and diode lasers
26.
• Deep sclerectomy:This procedure involves elevating a partial-
thickness scleral flap and removing the external portion of the
Schlemm canal and outer part of the trabecular meshwork, including
juxtacanalicular tissue, without fully penetrating the eye, thus less risk
of hypotony and endophthalmitis.
27.
Penetrating Keratoplasty
• Reservedfor patients with severe visual disability whose glaucoma is
well controlled.
• Optical iridectomy - less risky procedure
28.
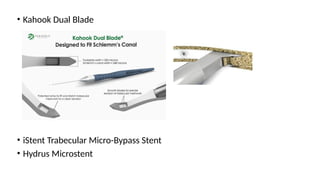
MIGS in PCG
•Gonioscopy-assisted transluminal trabeculotomy (GATT)
• Trab360 and Omni devices




























![Adult glaucoma surgery da luz, freitas maria [srg]](https://cdn.slidesharecdn.com/ss_thumbnails/adultglaucomasurgery-daluzfreitasmariasrg-150513044555-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
























