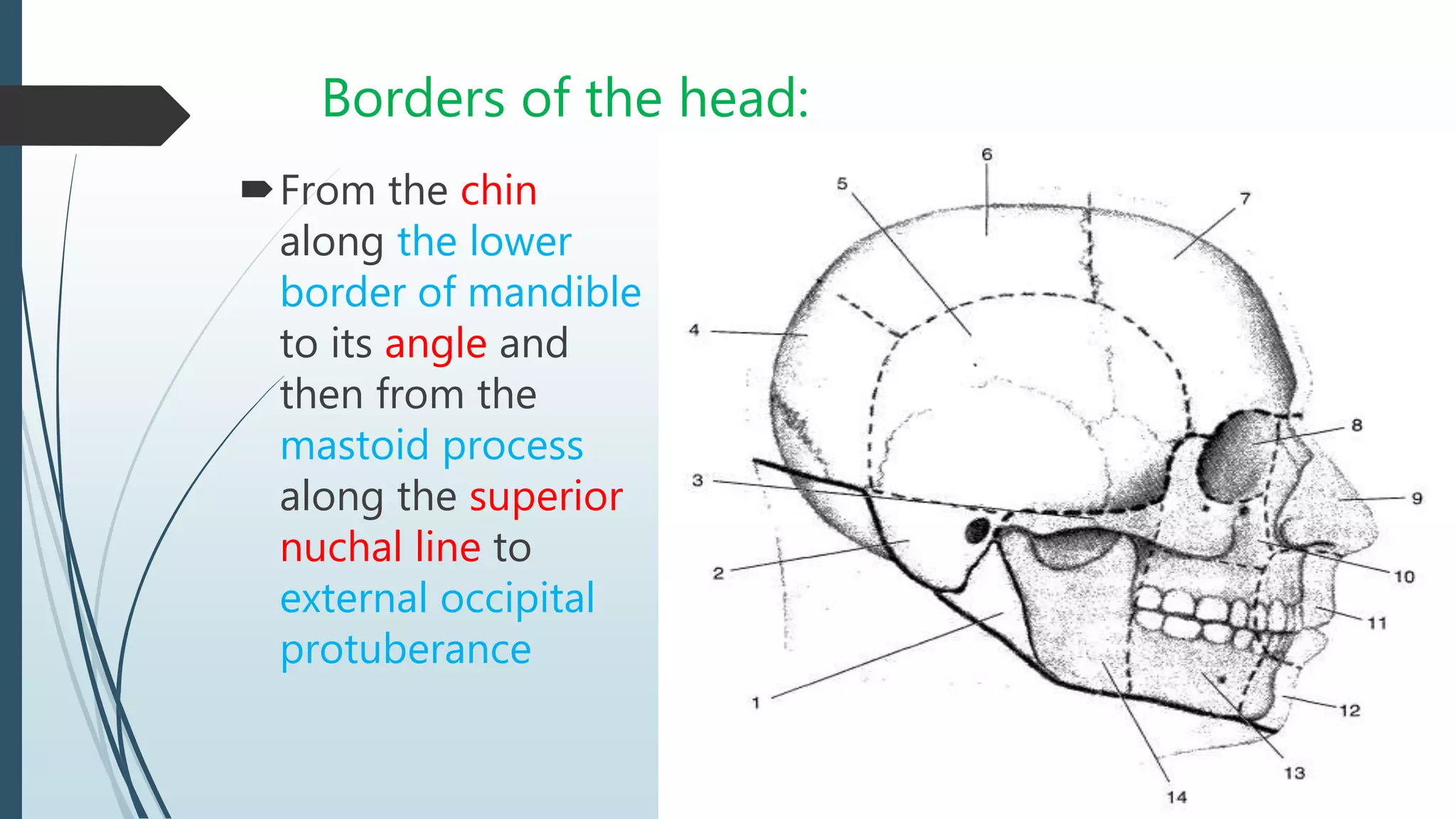
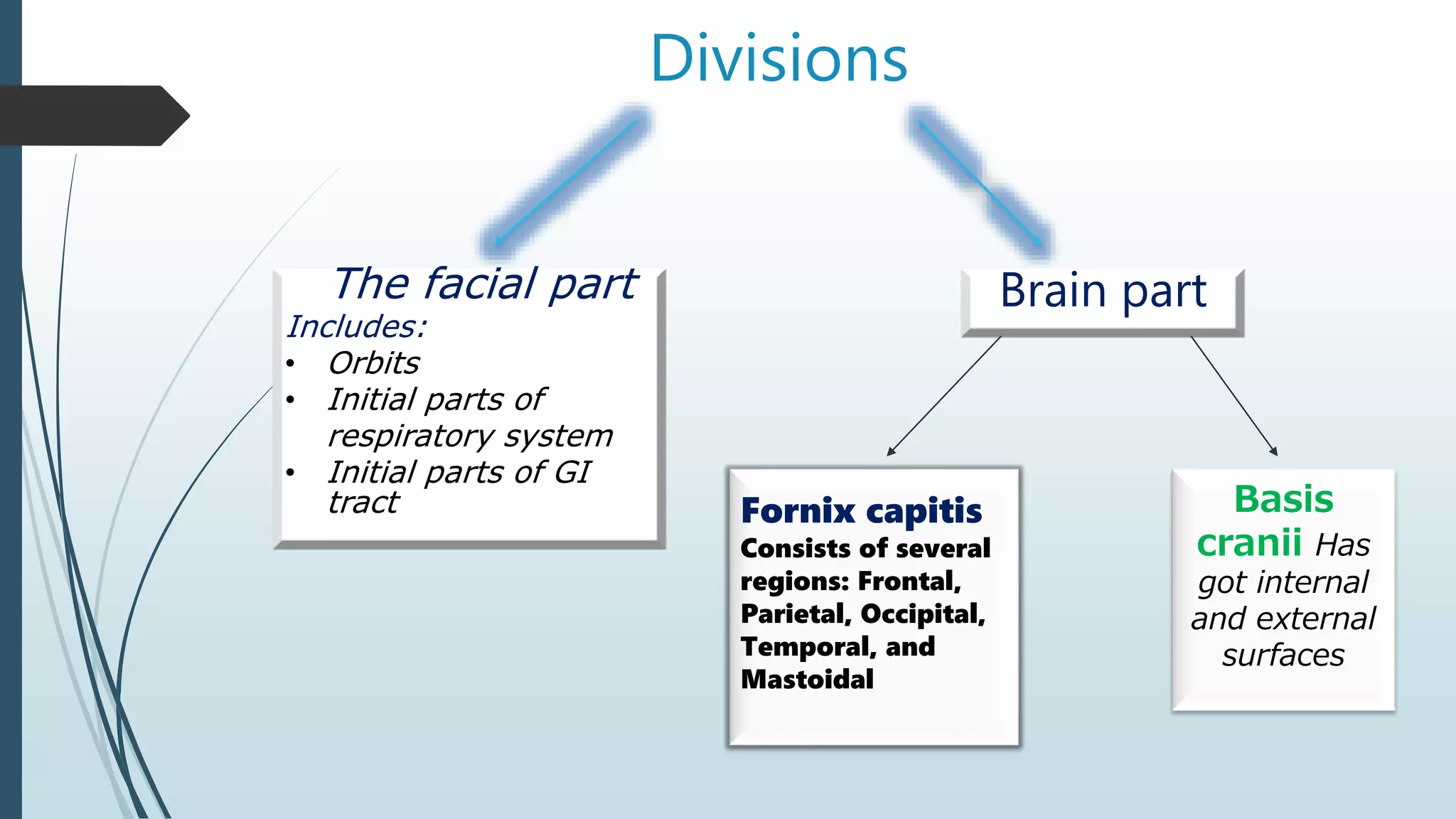
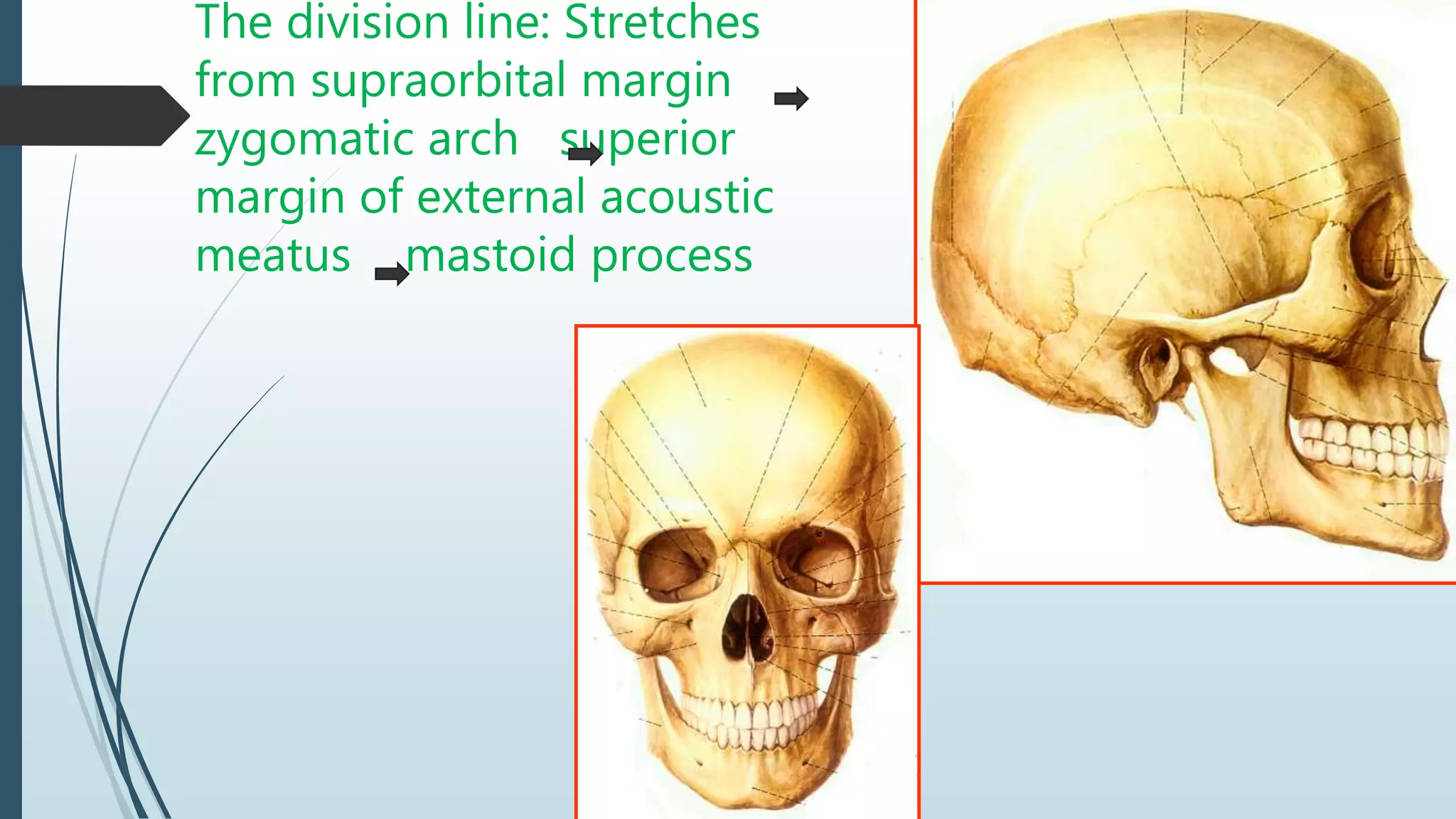
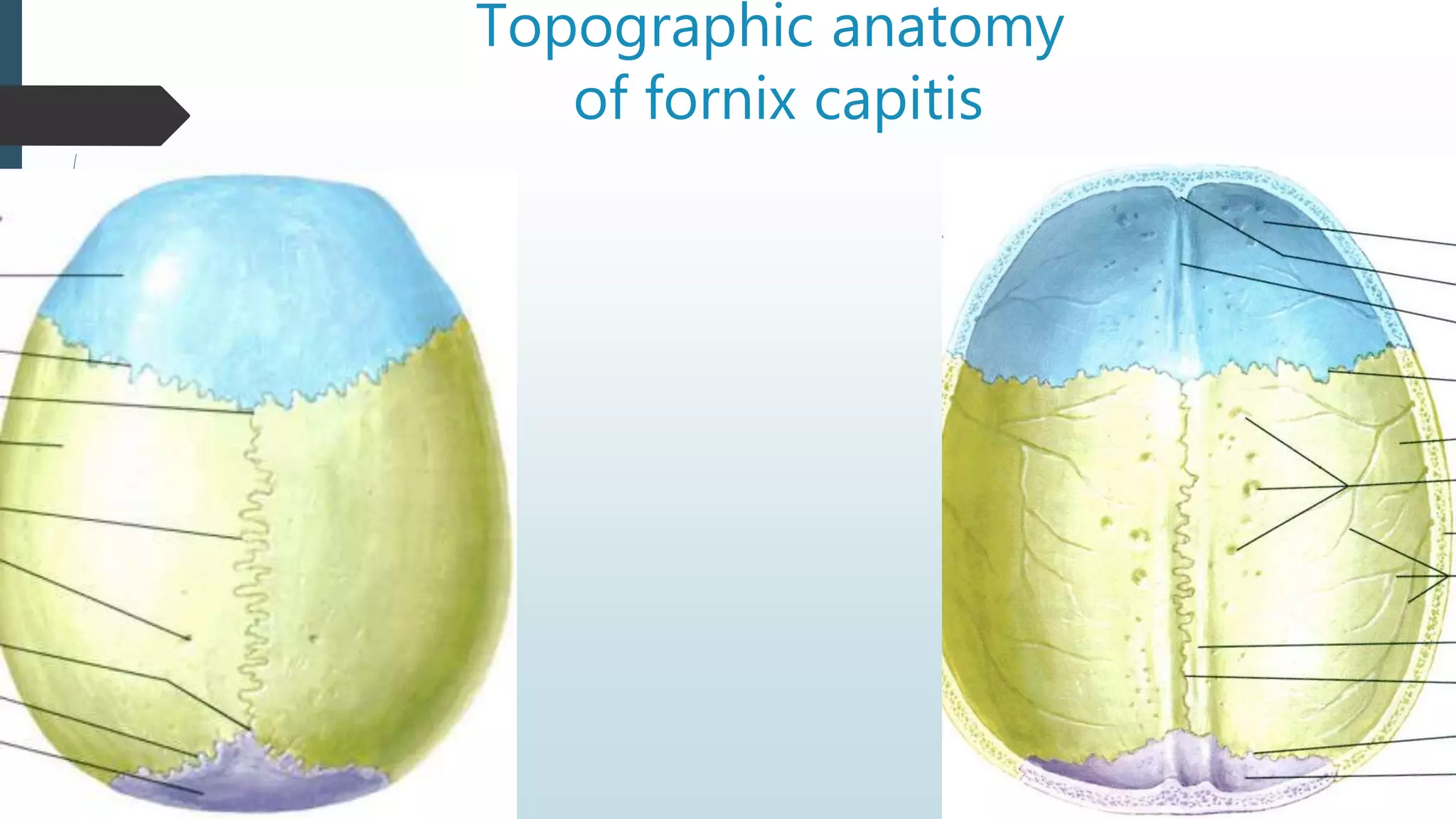
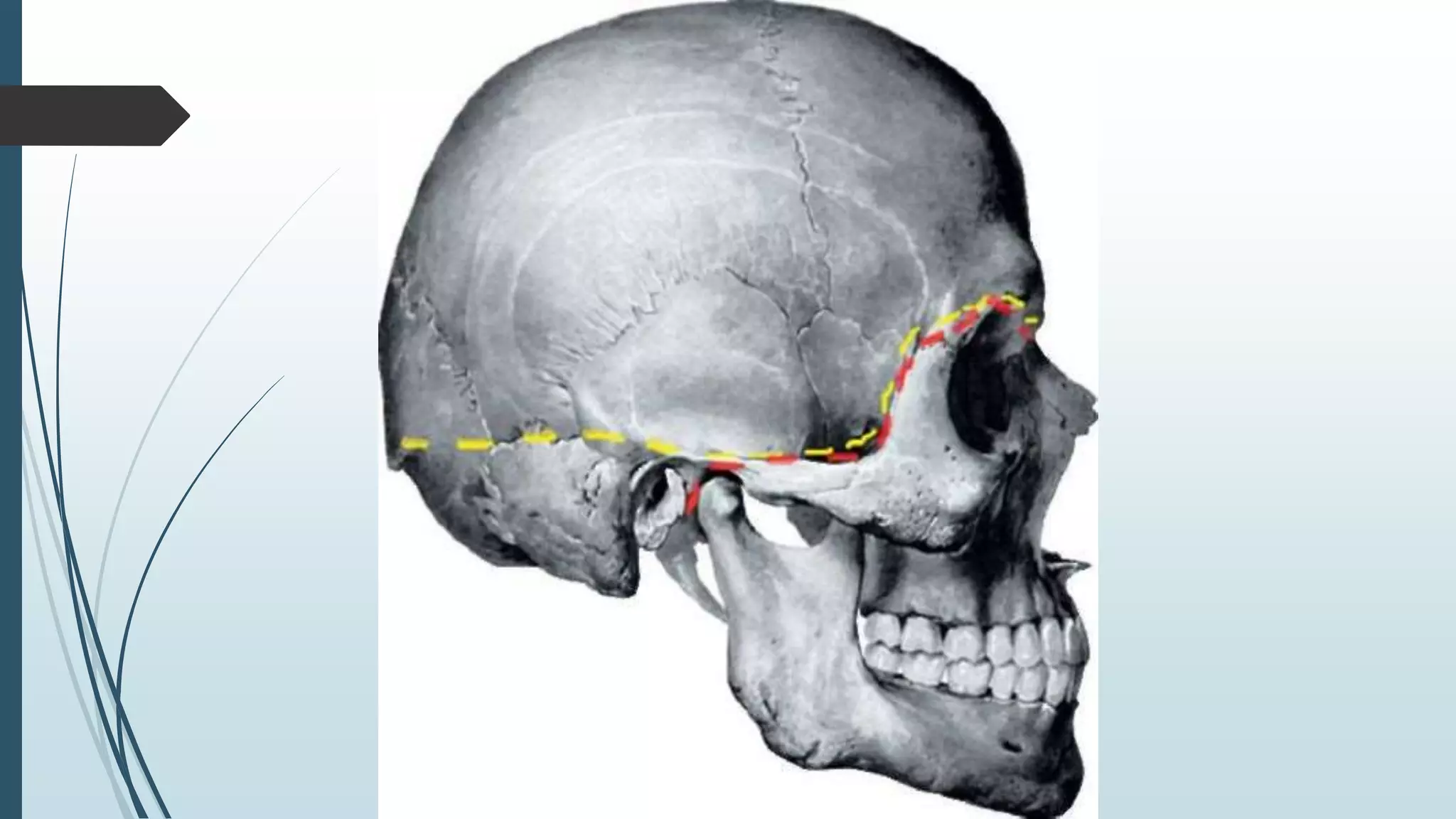
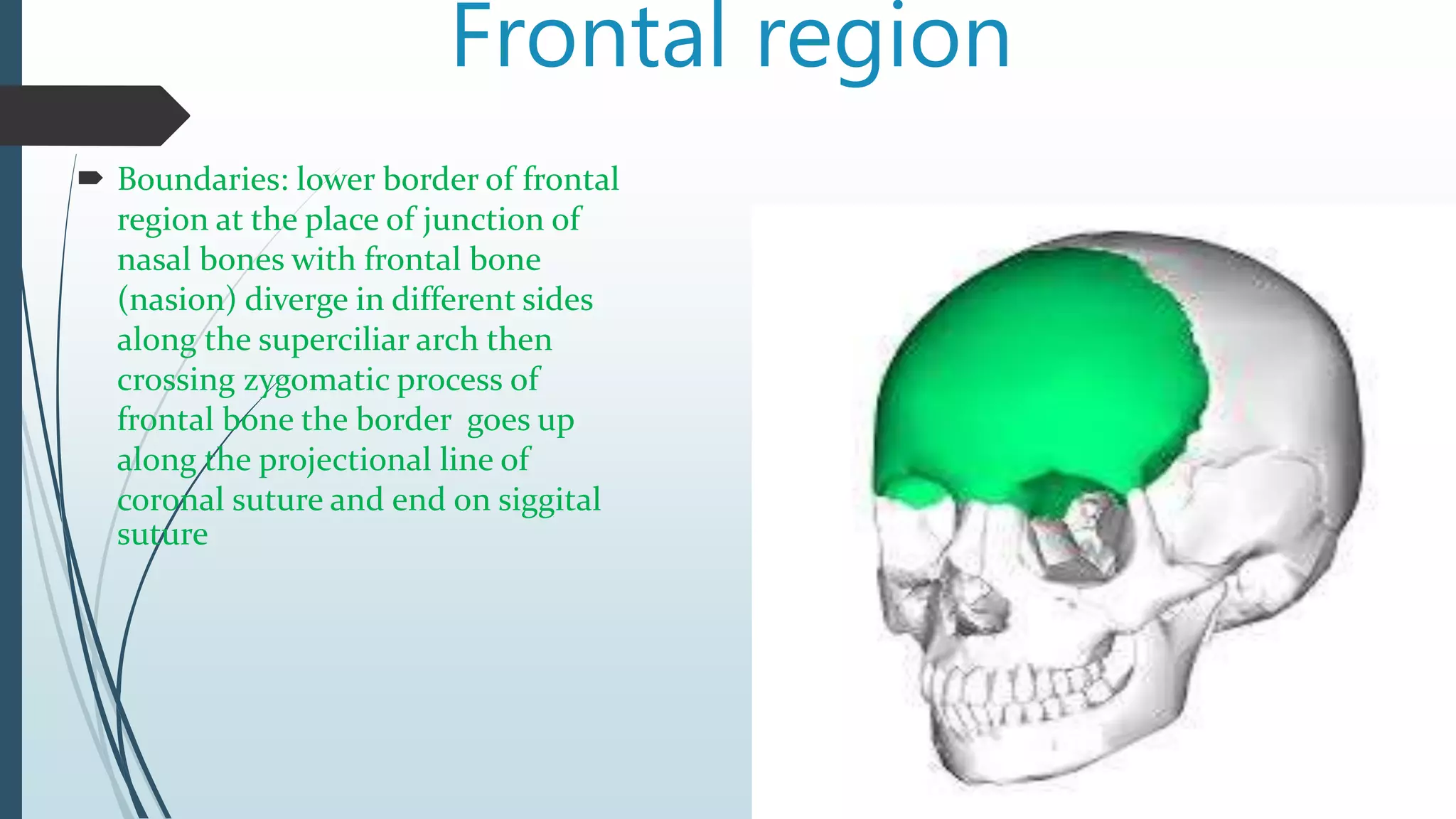
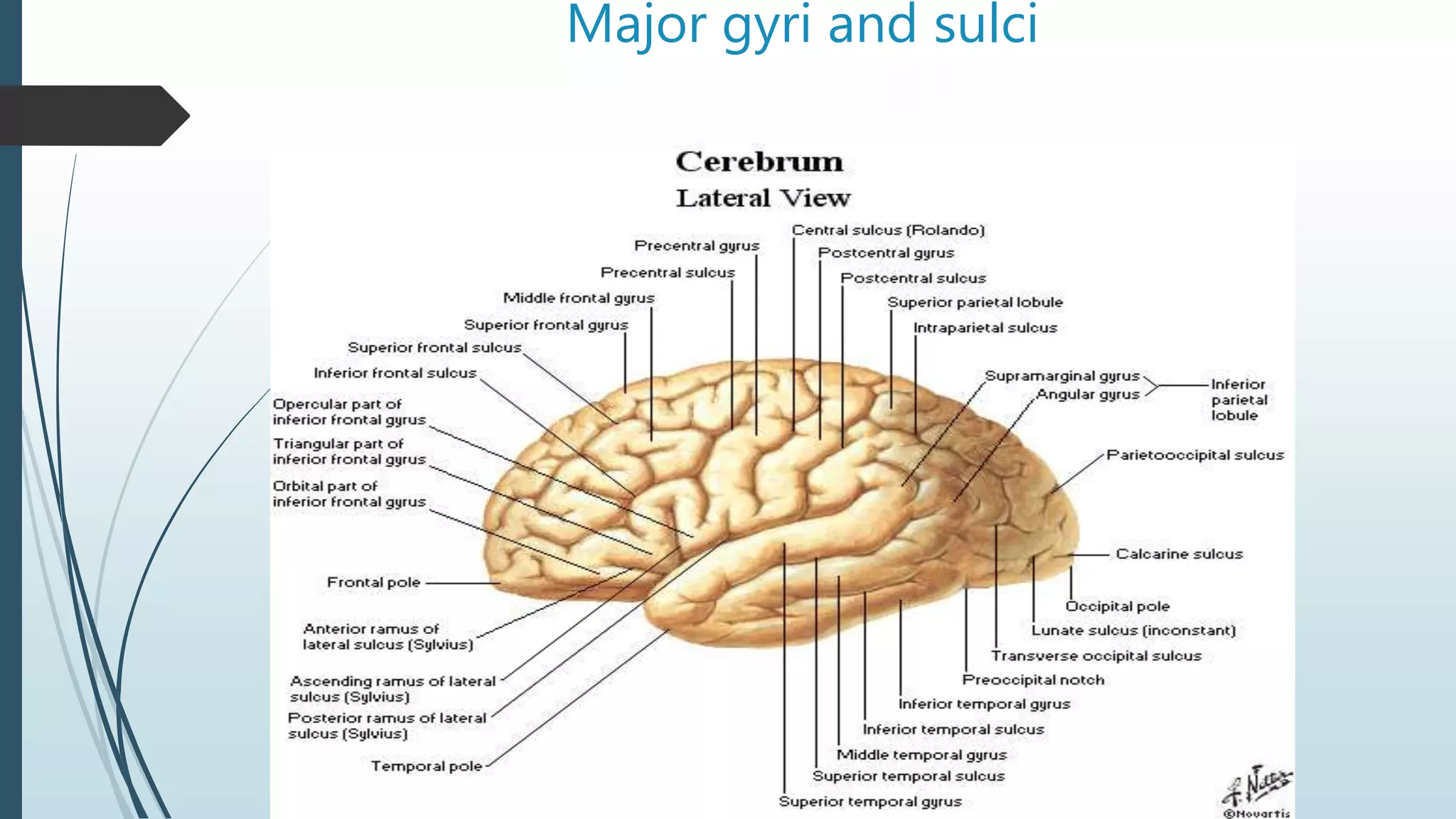
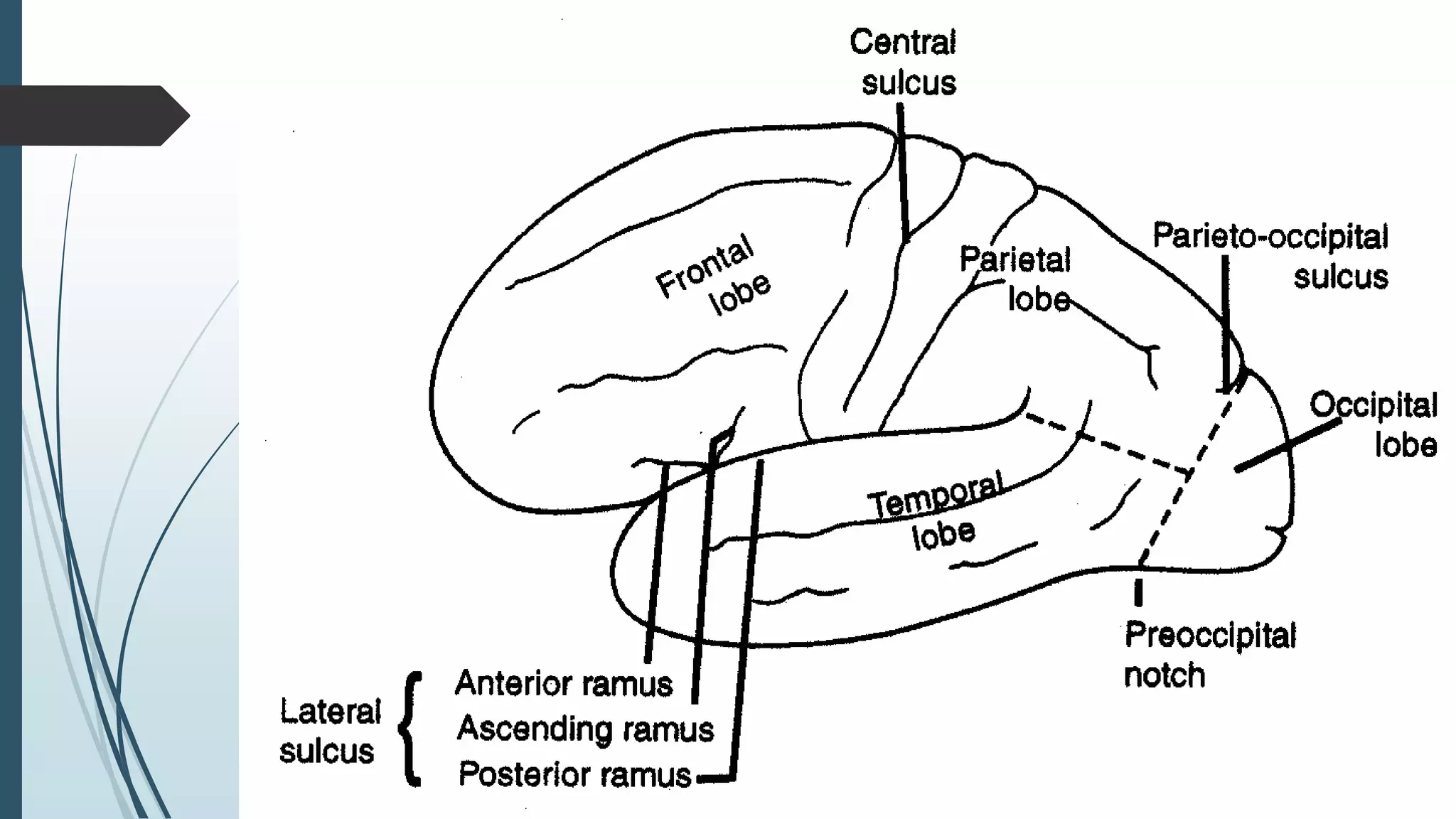
This document provides a summary of the topographic anatomy of the brain and skull. It describes the boundaries and divisions of the head and skull. It then discusses the layers and structures of the meninges (membranes) covering the brain, including the dura mater, arachnoidea, and pia mater. It also outlines the four ventricles within the brain and describes their connections. Major gyri (convolutions) and sulci (fissures) of the brain are identified. The four main lobes of the brain - frontal, parietal, temporal and occipital - are also defined based on distinguishing anatomical features.









































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












