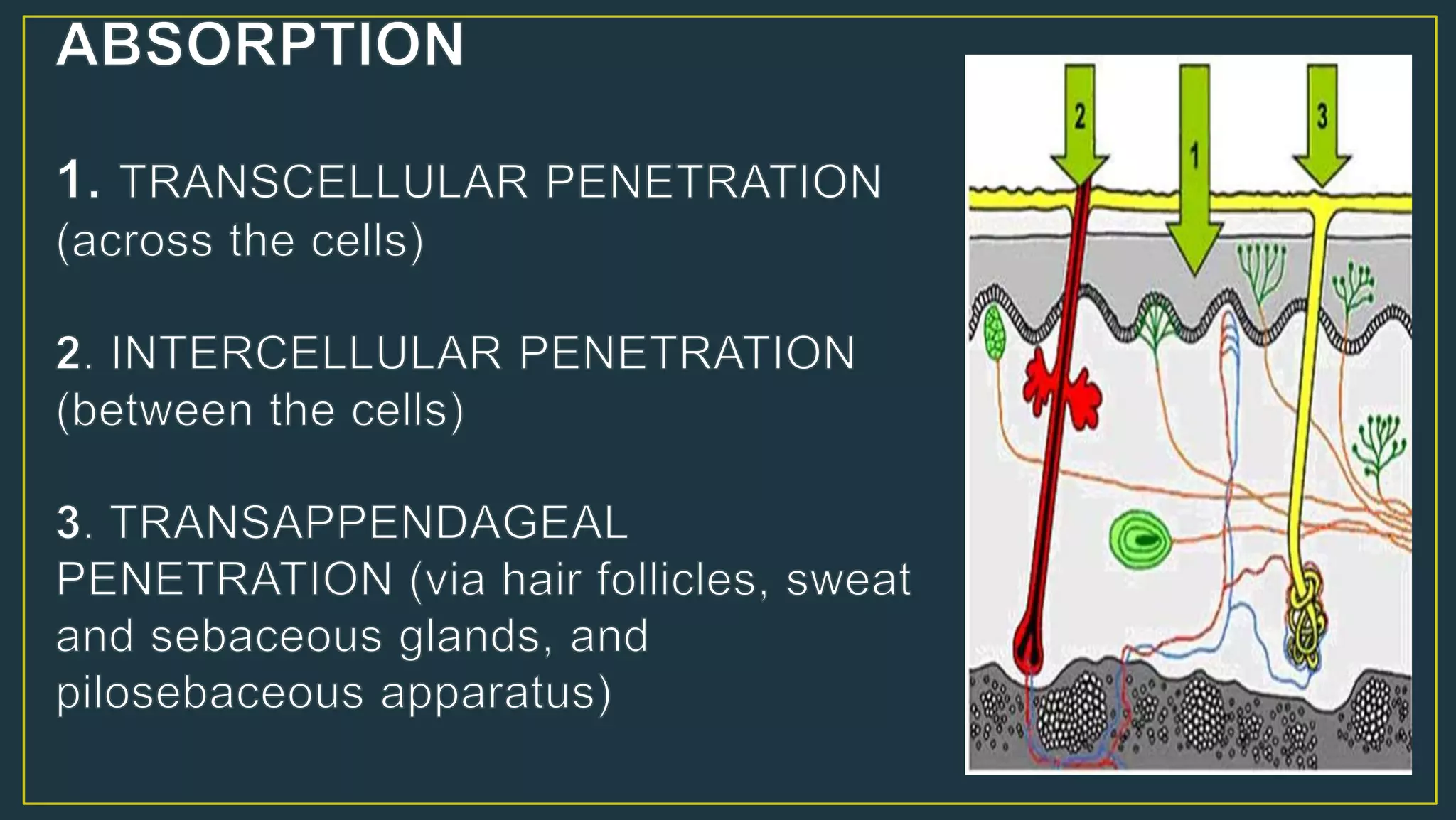
This document provides information on topical drug delivery and formulations. It defines a topical medication as one applied to the skin or mucous membranes, allowing high drug concentration locally with minimal systemic exposure. Topical absorption is influenced by stratum corneum thickness and is highest in mucous membranes and lowest in skin areas like the soles and dorsa of hands/feet. Proper dosing of a topical medication considers factors like concentration, application frequency, site, and occlusion. Occlusion can increase drug delivery by 10-100 times by hydrating the skin. The document then discusses various topical formulations like solutions, suspensions, emulsions, gels, ointments, creams, powders and their characteristics.