Downloaded 43 times

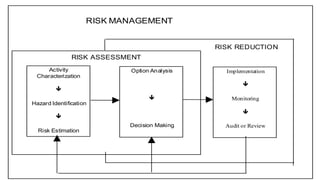
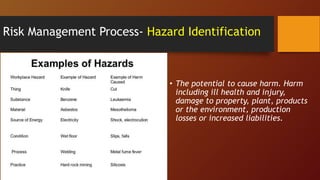


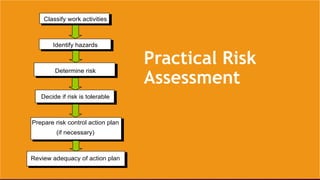


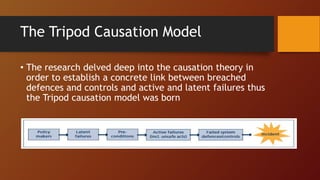


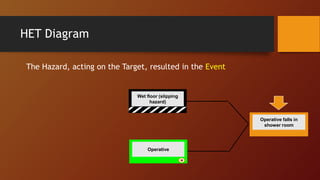
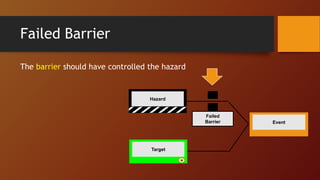
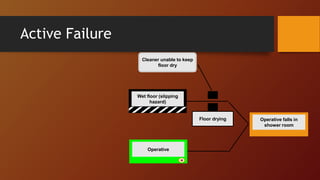
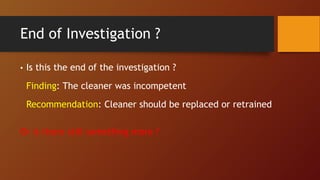
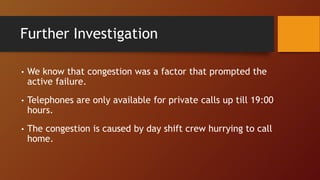
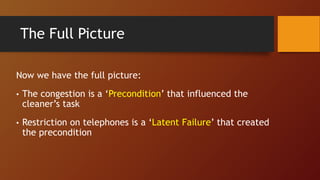
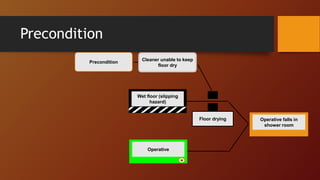
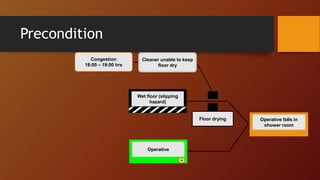
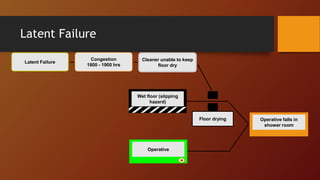
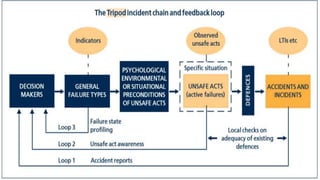


The document provides an overview of risk management principles and processes for human error. It discusses qualitative and quantitative risk assessment approaches. The key stages of risk management are identified as hazard identification, risk assessment, and risk control. Methods for hazard identification, risk estimation, and developing risk control plans are outlined. Finally, the TRIPOD framework for accident investigation and analysis is introduced, which uses a causal model to identify hazards, events, targets, barriers, failures, preconditions, and latent failures.



















![Riskass06[1]](https://cdn.slidesharecdn.com/ss_thumbnails/riskass061-100906114112-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)

