Download as PDF, PPTX
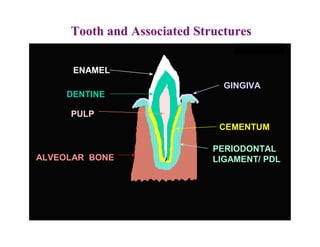
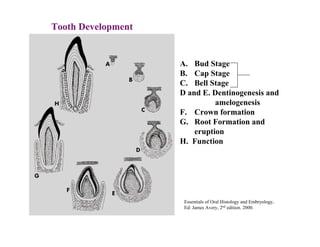
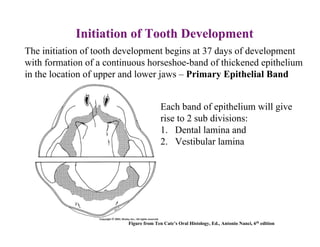
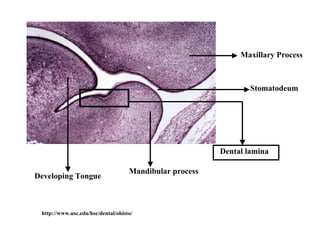
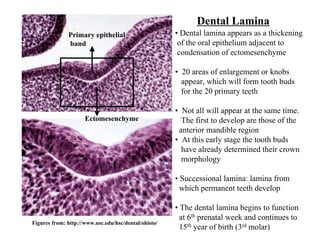
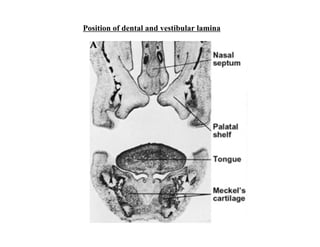
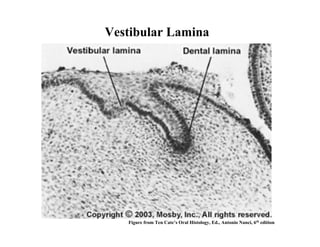
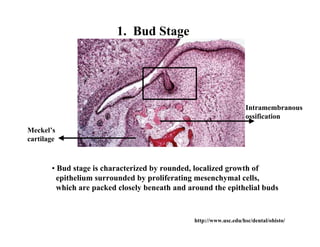
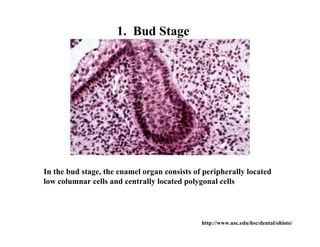
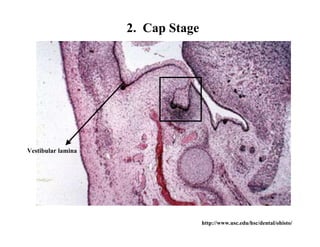
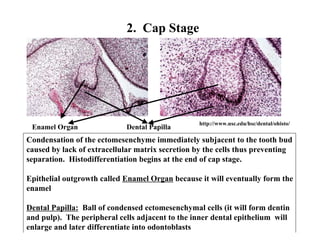
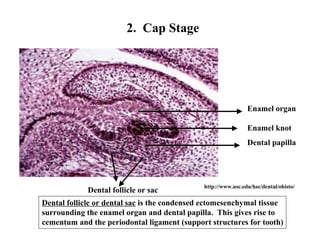
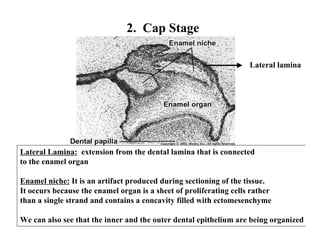
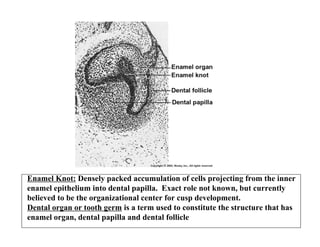
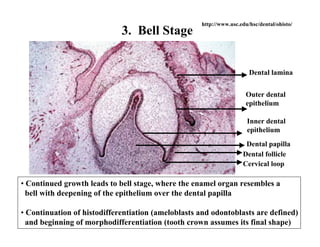
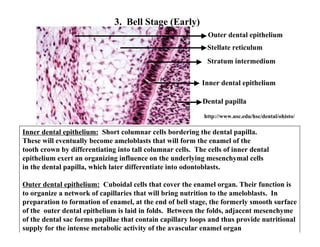
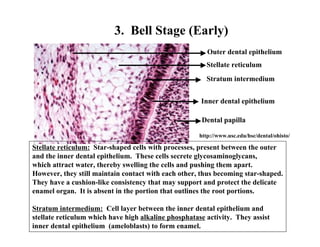
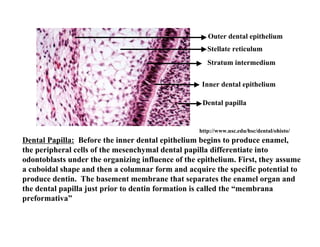
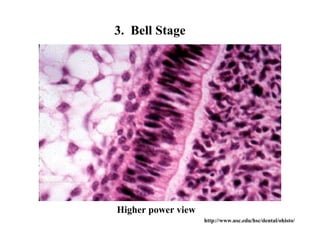
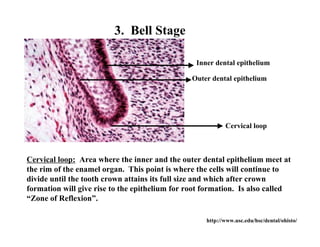
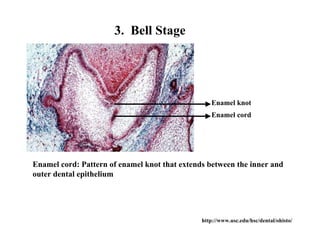
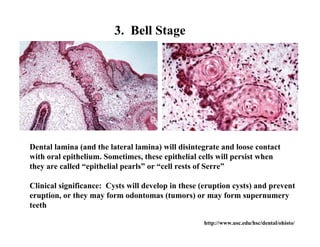
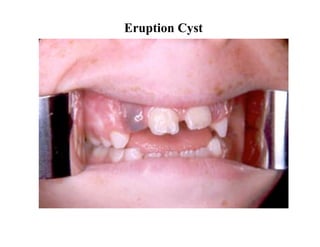
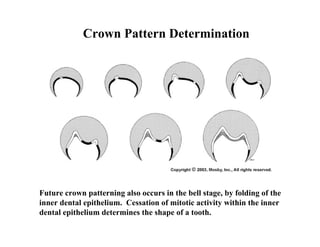
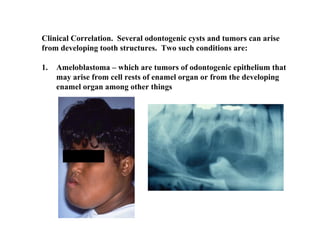
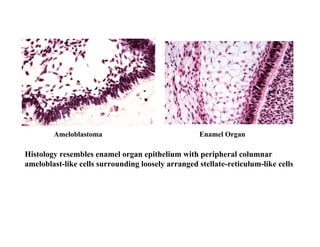
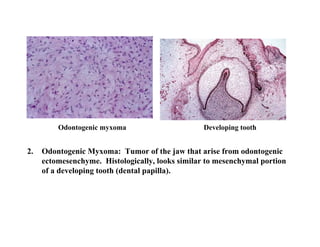
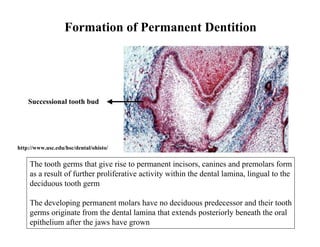
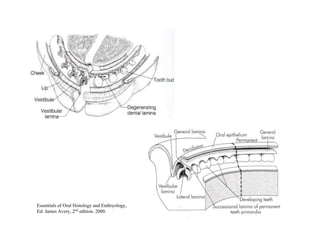
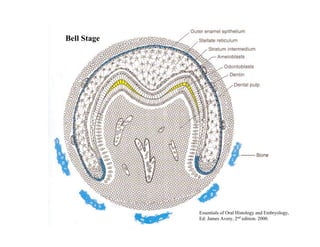
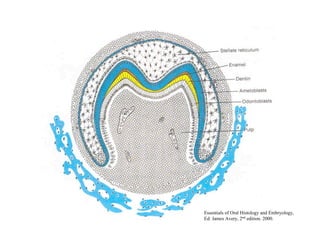
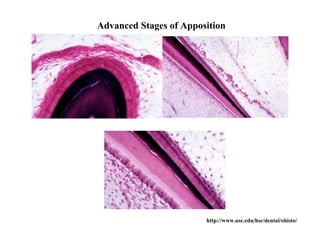
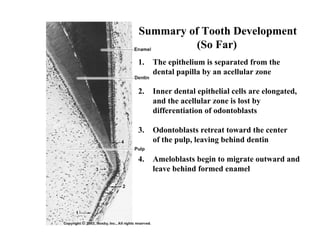
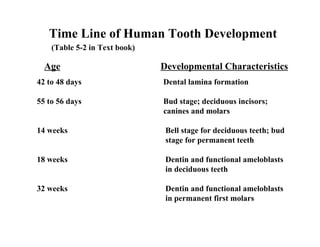
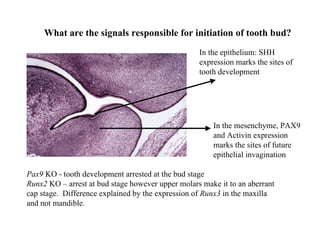

The document describes the development of teeth and supporting tissues. It discusses the initiation of tooth development from the primary epithelial band, the formation of the dental lamina and vestibular lamina. Tooth development occurs in 3 stages: the bud stage is characterized by localized epithelial growth, the cap stage shows epithelial outgrowth forming the enamel organ and dental papilla, and the bell stage resembles a bell shape with deepening epithelium over the dental papilla and histodifferentiation of ameloblasts and odontoblasts. The enamel organ and dental papilla develop further in the bell stage in preparation for enamel and dentin formation.




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















