- Tooth eruption is the movement of teeth through the gums and bone to appear in the mouth and allow for proper function.
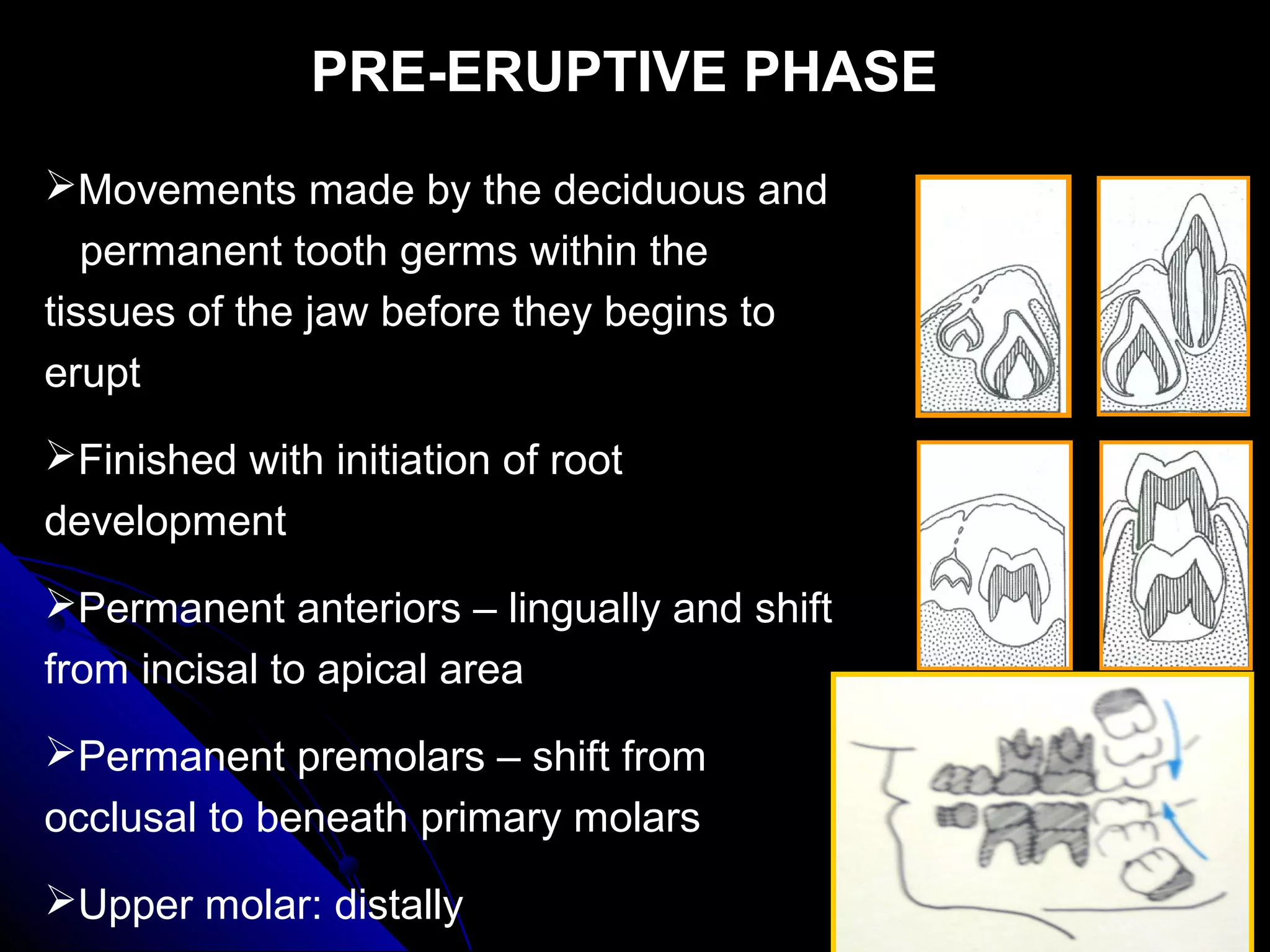
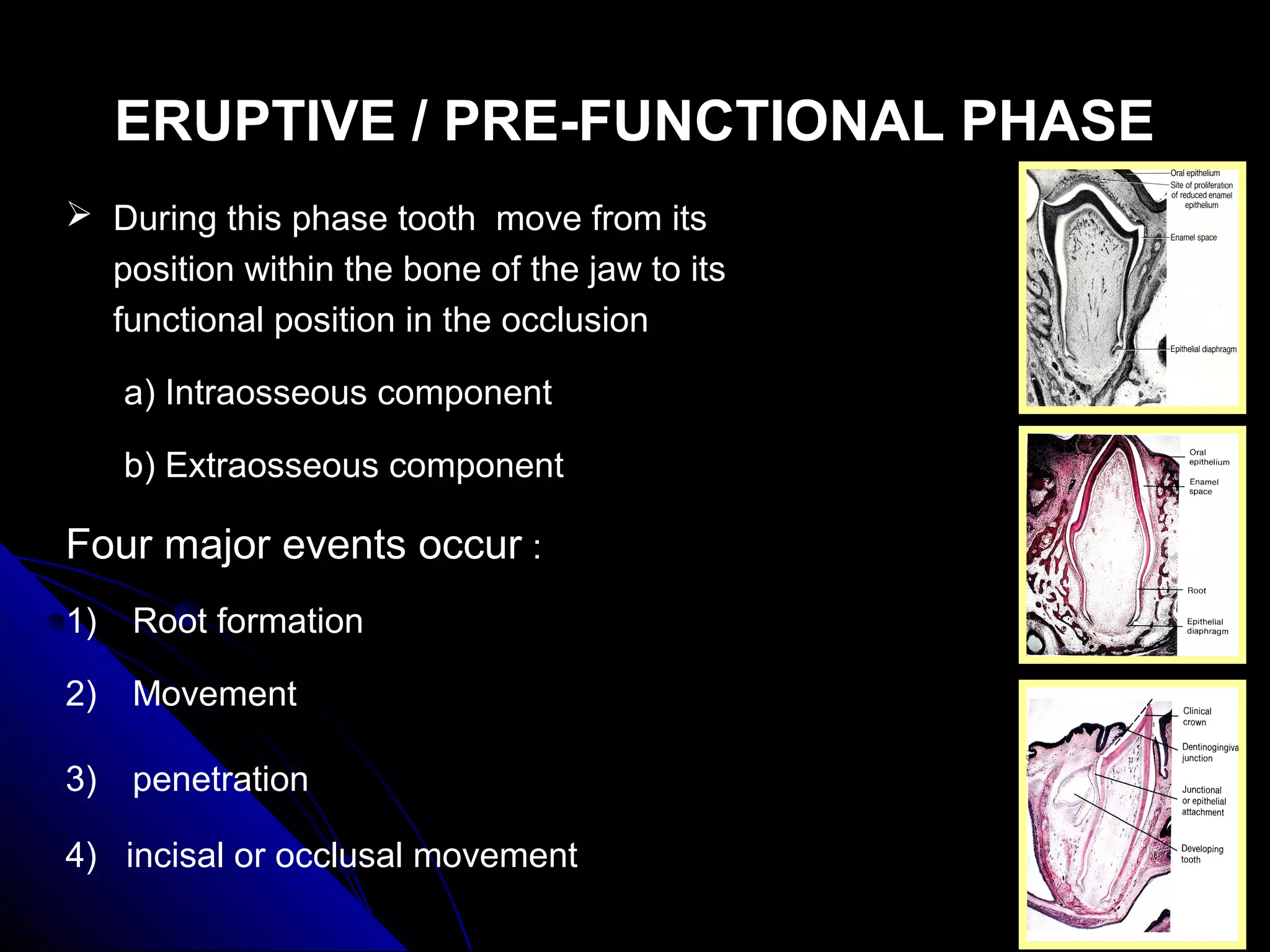
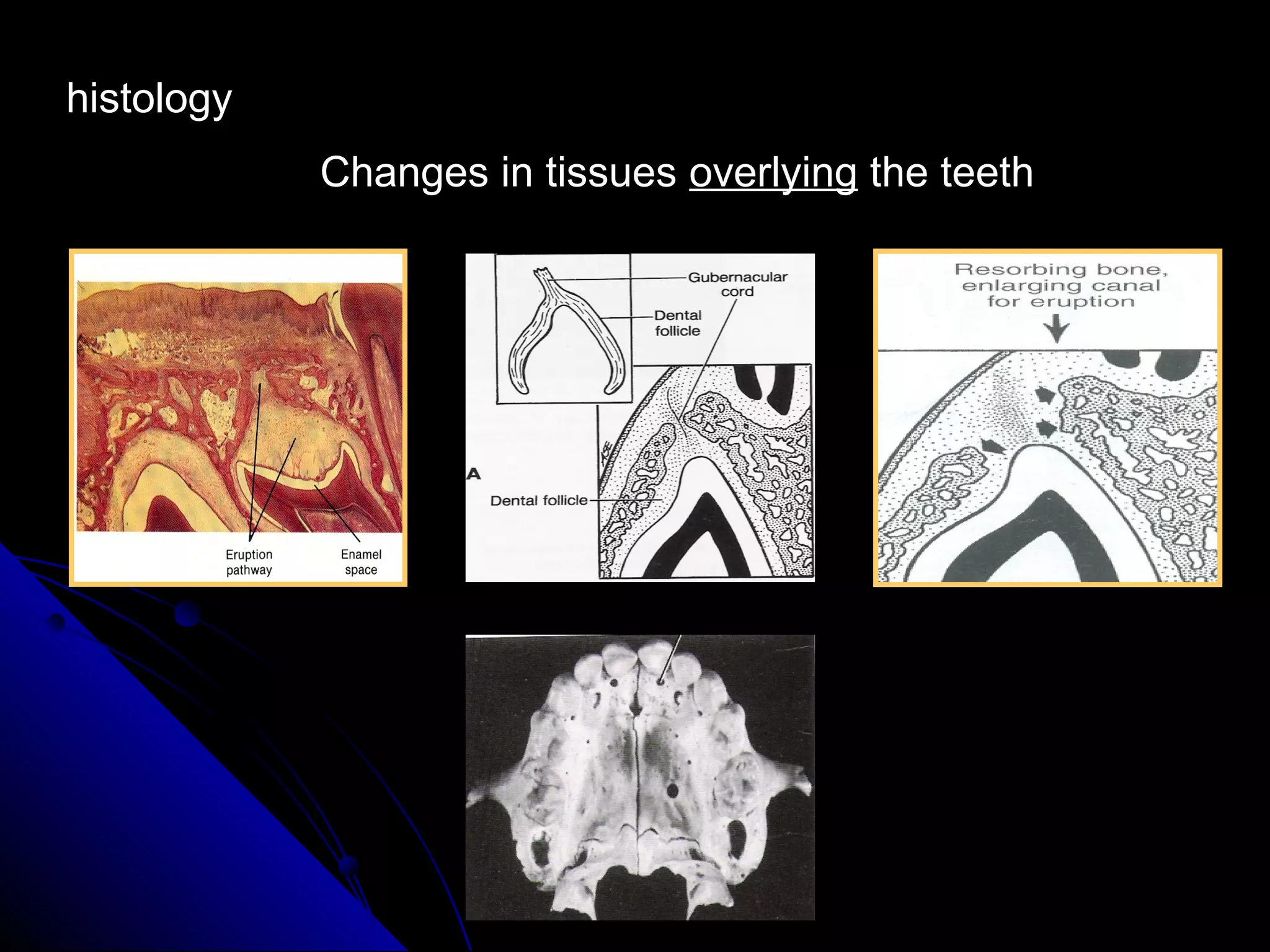
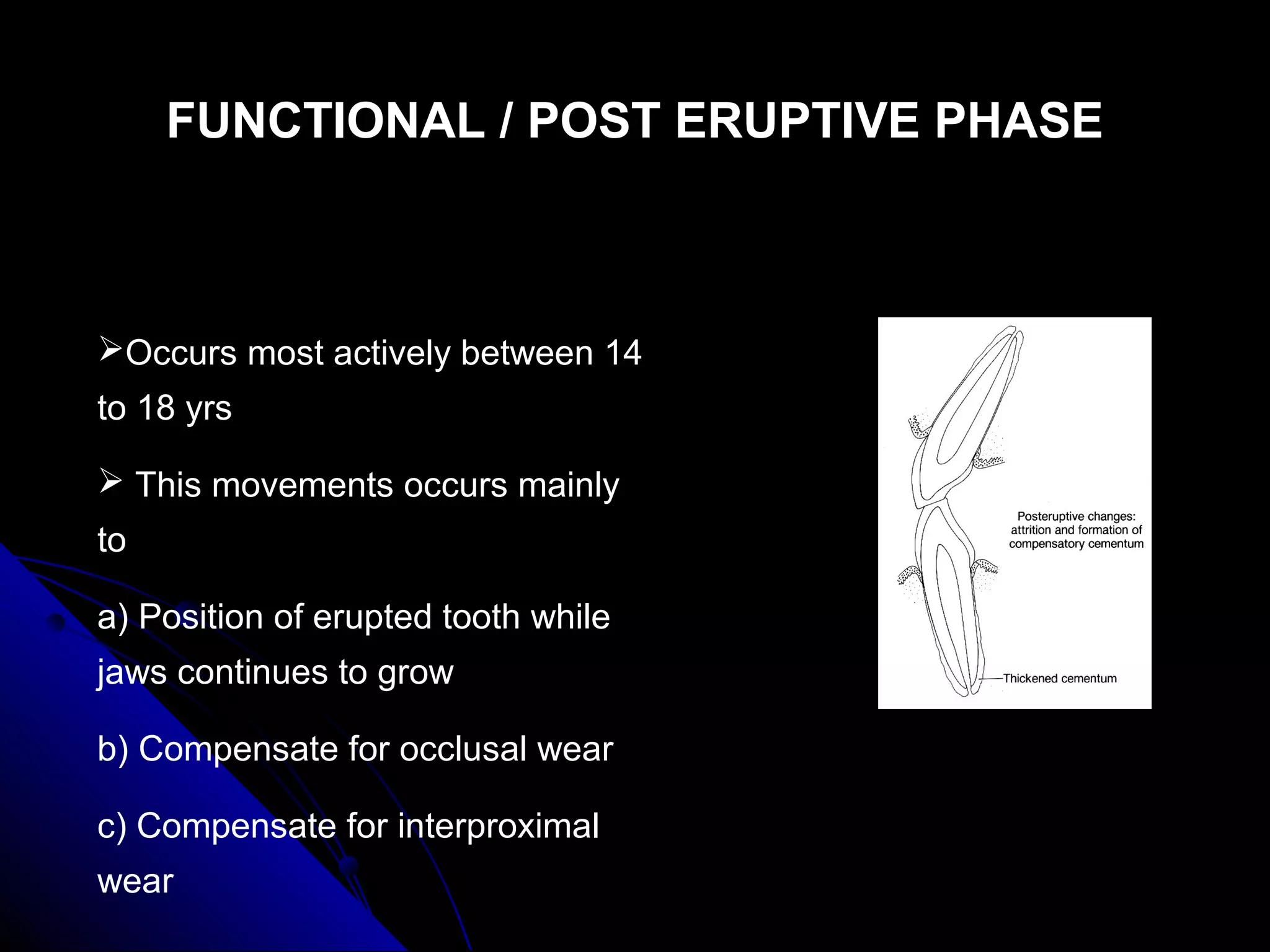
- It occurs in three phases: pre-eruptive within the bone, eruptive as it emerges through the gums, and posteruptive as it aligns fully.
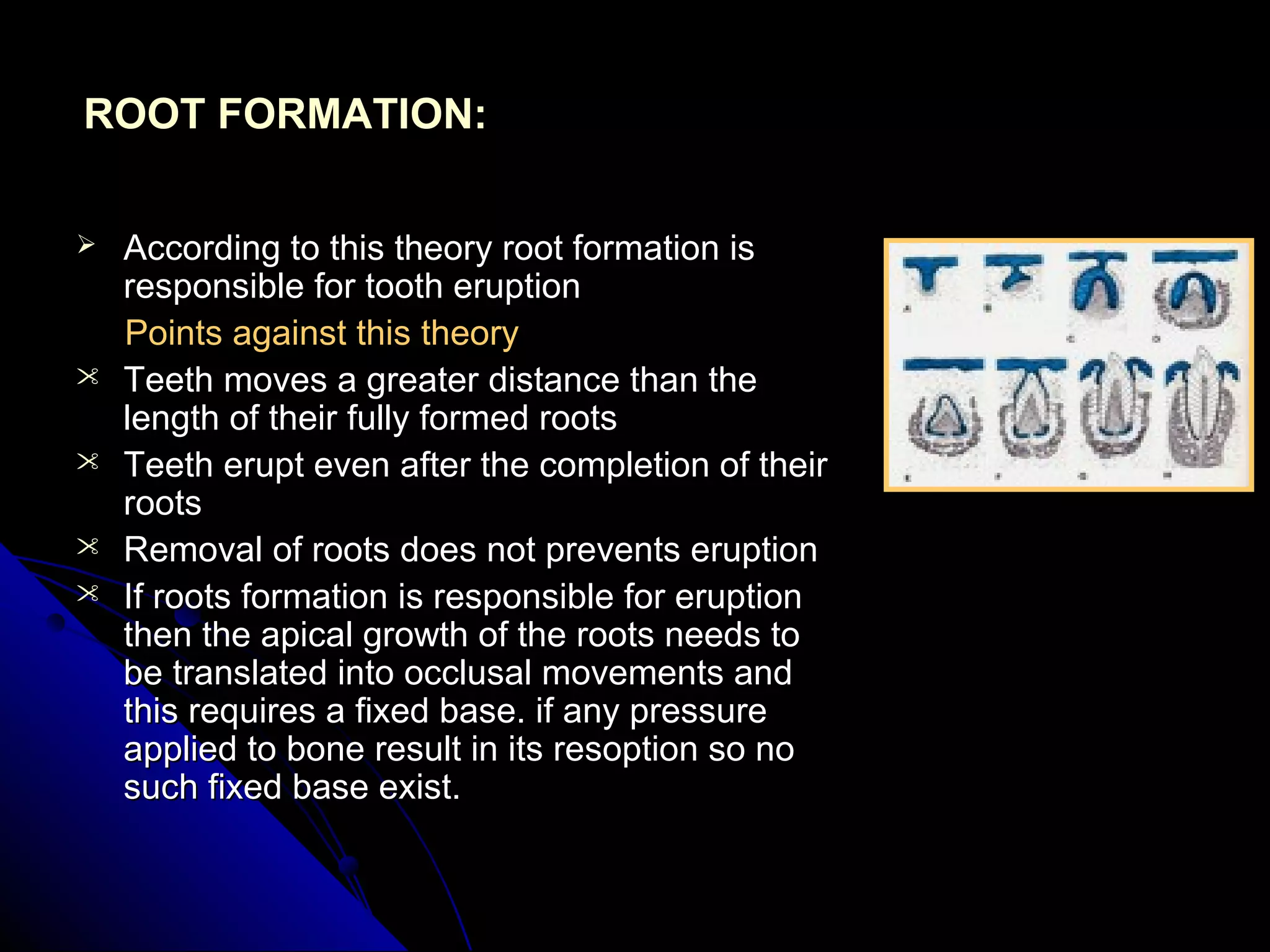
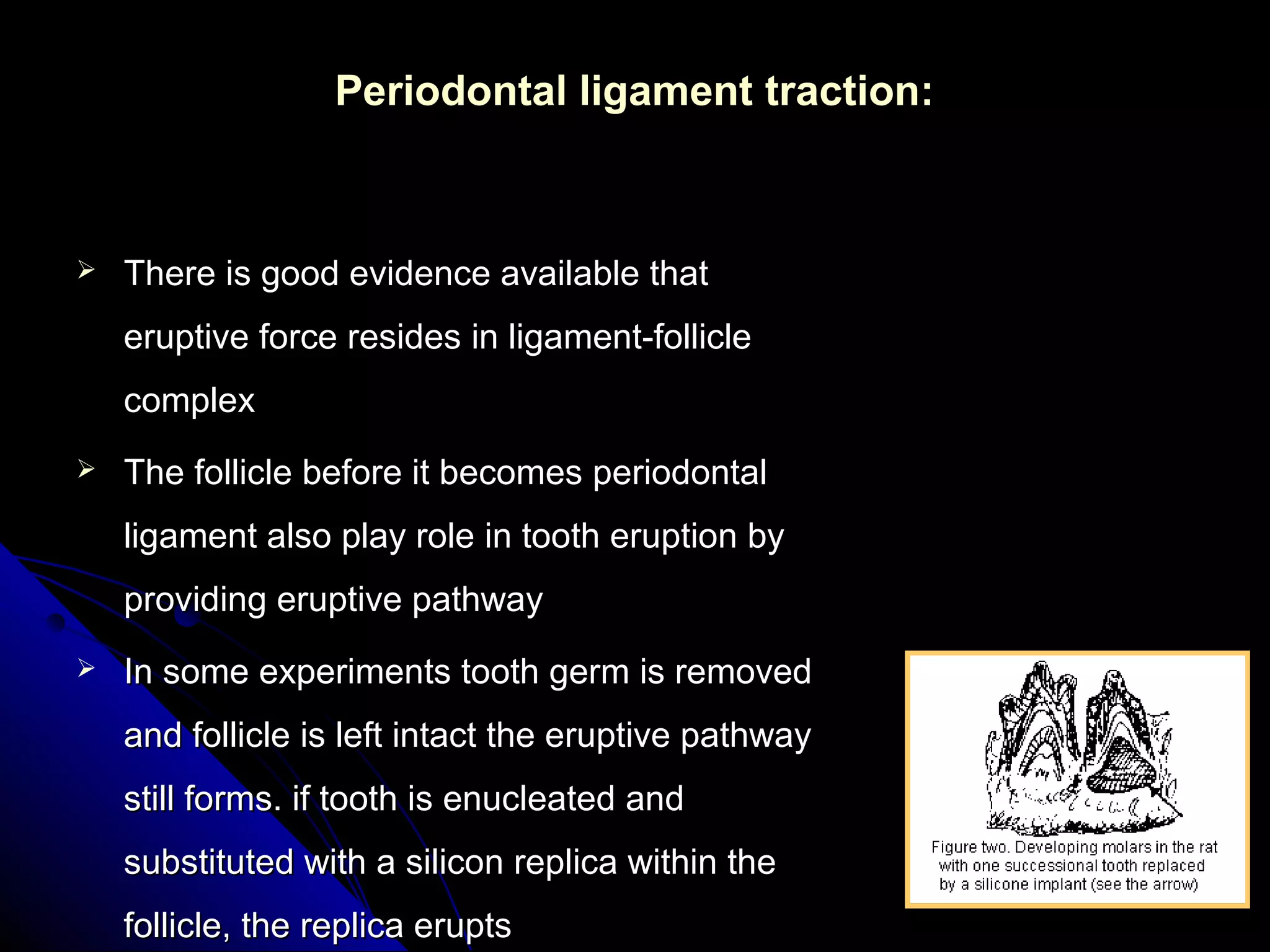
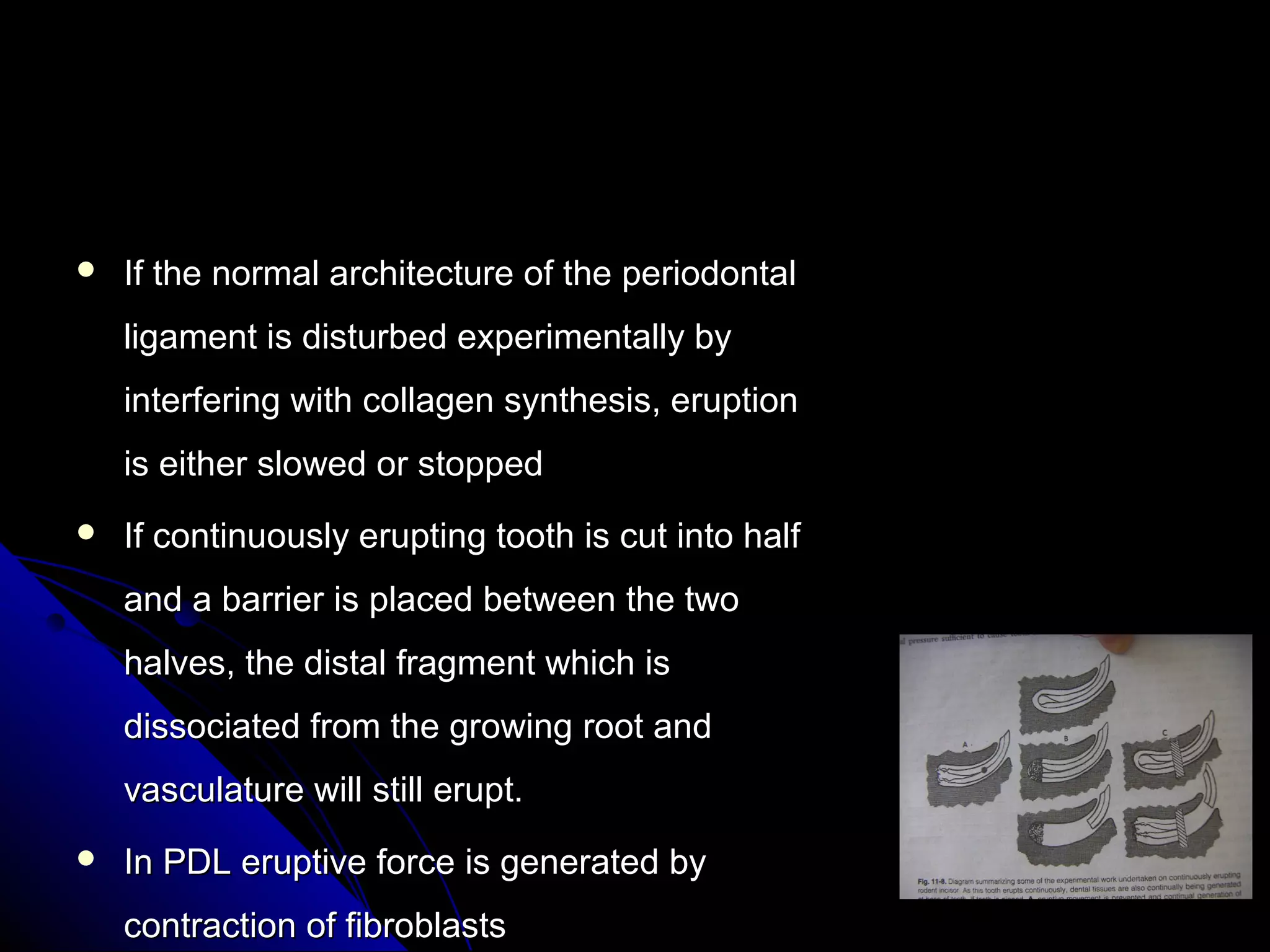
- Several theories exist for the mechanism of eruption including root formation, vascular pressure, and periodontal ligament traction which recent evidence supports as the driving force.