Downloaded 784 times
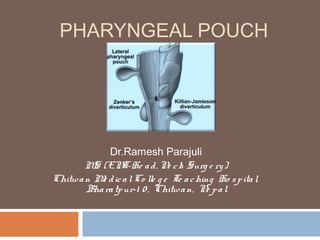
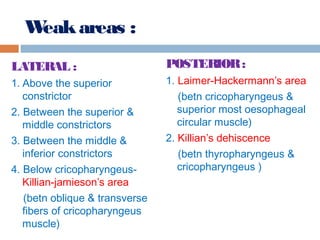
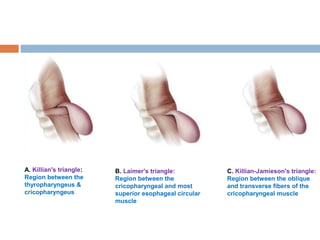
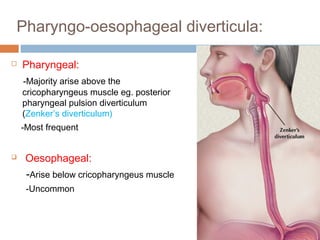
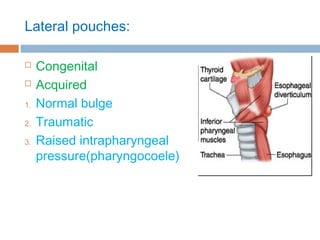
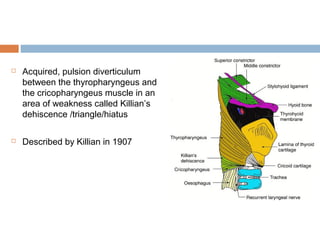
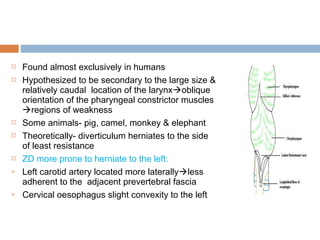
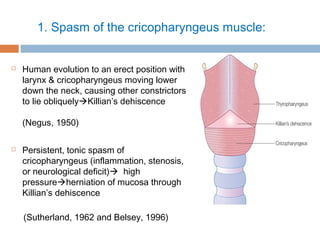
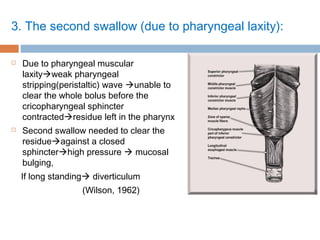
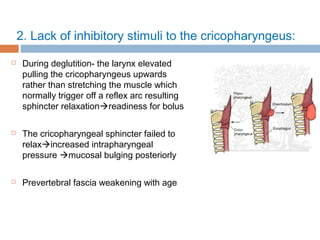
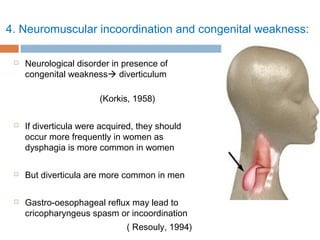
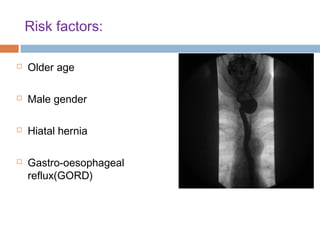

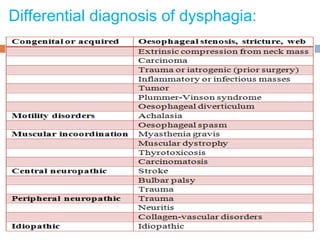
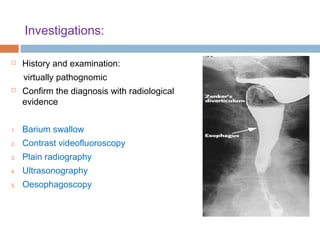
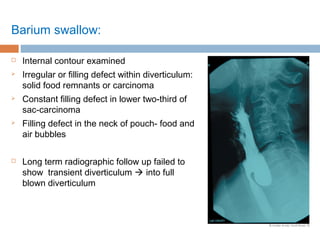
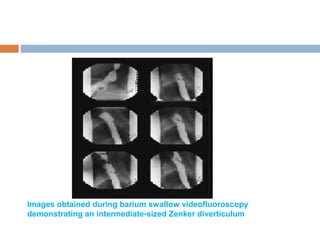
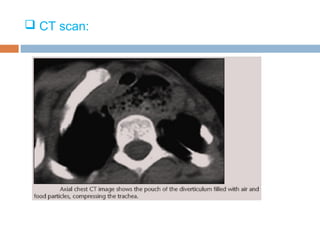


Pharyngeal pouch, also known as Zenker's diverticulum, is a pulsion diverticulum that arises between the thyropharyngeus and cricopharyngeus muscles in an area of weakness. It is the most common type of posterior pharyngeal pouch. Zenker's diverticulum usually presents in older adults, affecting men more often than women. Symptoms include dysphagia, regurgitation of food, and halitosis. Treatment involves surgical excision of the diverticulum. While the exact cause is unknown, it is hypothesized to be related to the large size and oblique orientation of the pharyngeal muscles in humans, creating regions of weakness where the divert





































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
