Downloaded 74 times

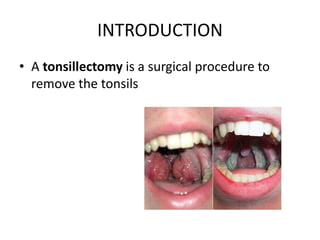
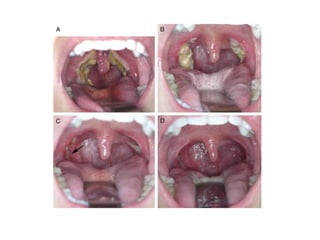

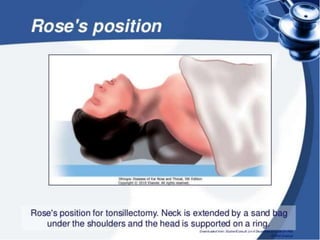
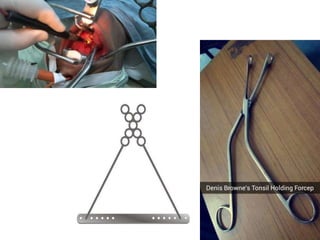

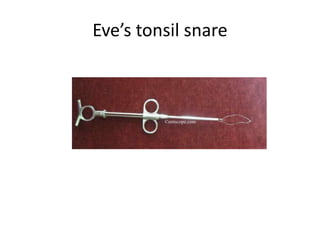
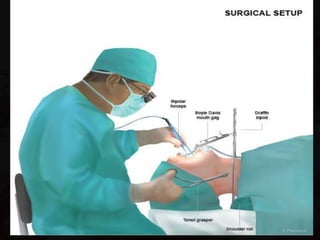

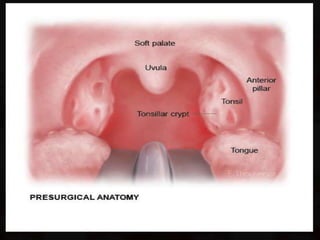
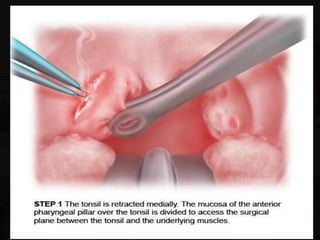
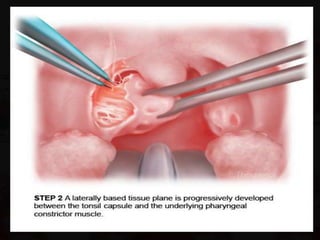
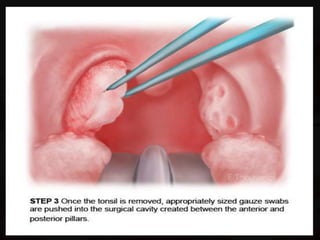

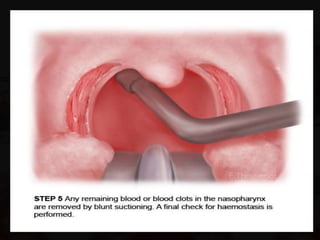
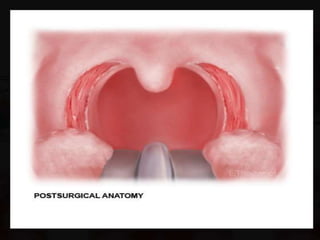


A tonsillectomy is a surgical procedure to remove the tonsils. It is usually performed under general anesthesia with the patient in the Rose's position. The surgery involves using a mouth gag, grasping the tonsil with forceps, and dissecting it from the surrounding tissue using scissors or a dissector. A wire snare is then used to ligate and remove the tonsil. Post-operative care includes monitoring for bleeding, a soft diet, oral hygiene, analgesics and antibiotics. Complications can include bleeding, injury to nearby structures, infection, or scarring.























































































