This document discusses the anatomy, production, transport, regulation, and actions of thyroid hormones T3 and T4, including their biological activity and the importance of iodine intake. It outlines the mechanisms of thyroid hormone regulation by iodine levels and the hypothalamus/pituitary gland, as well as the consequences of thyroid hormone excess (hyperthyroidism) and deficiency (hypothyroidism) on various bodily functions. Additionally, it highlights the roles of thyroid hormones in growth, metabolism, cardiovascular health, and neurological development.

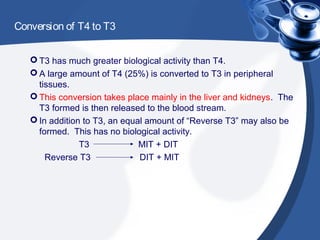

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





