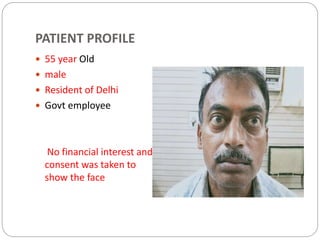
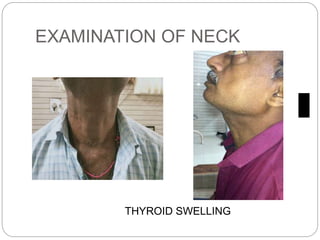
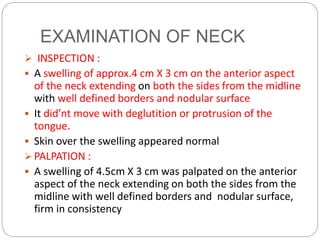
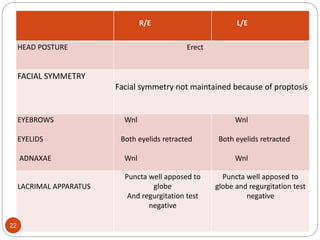
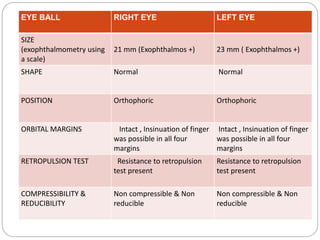
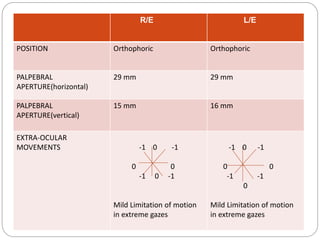
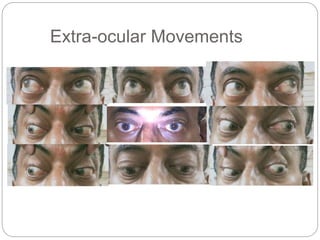
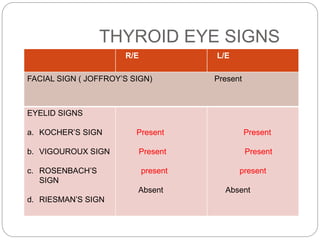
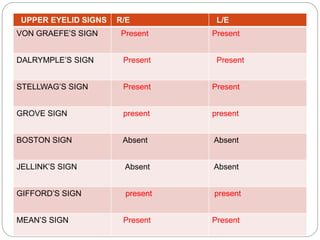
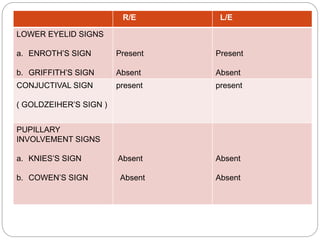
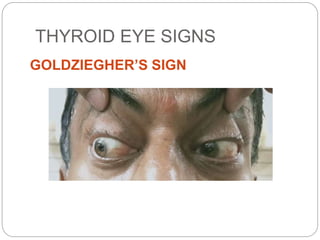
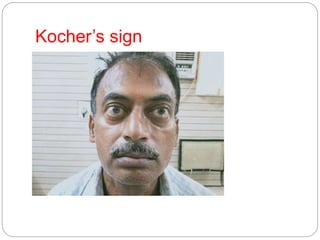
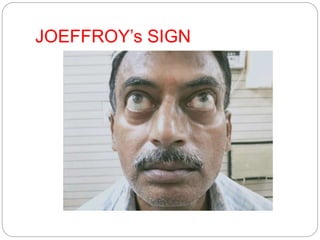
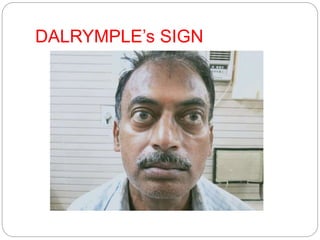
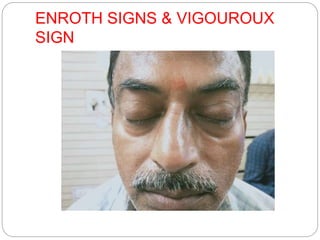
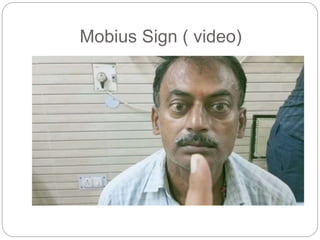
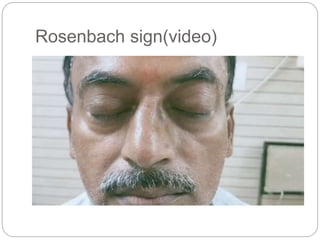
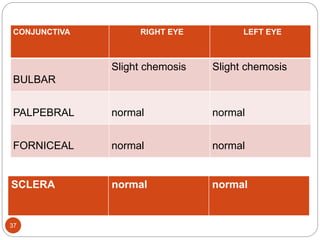
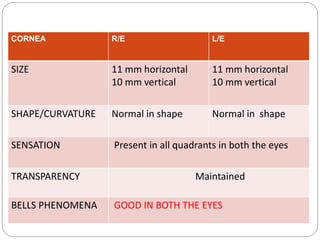
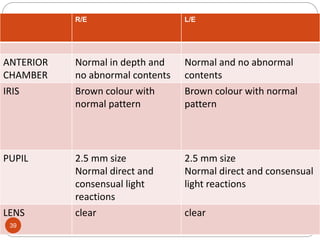
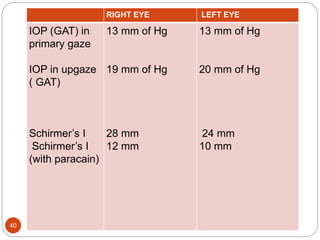
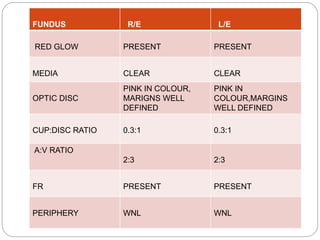
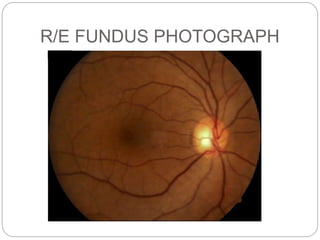
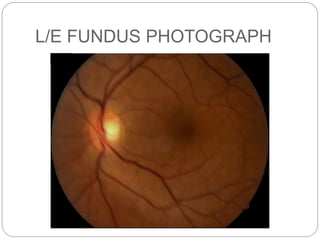
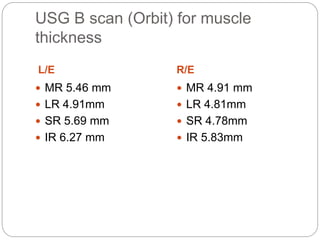
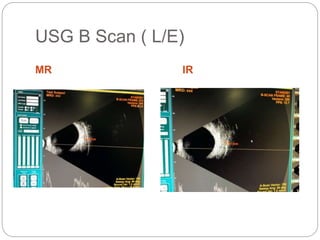
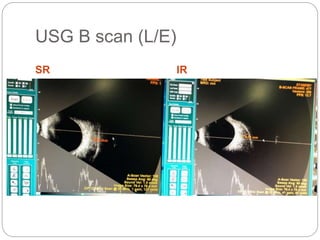
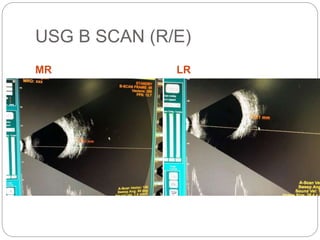
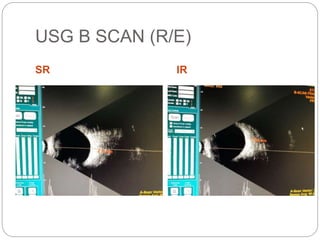
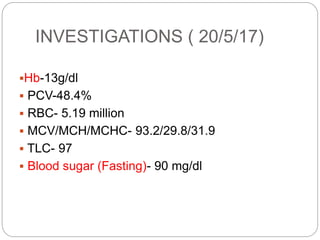
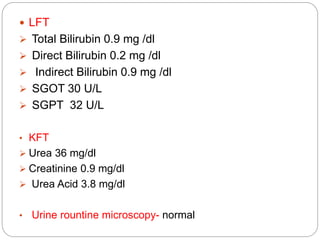
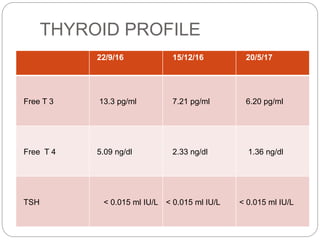
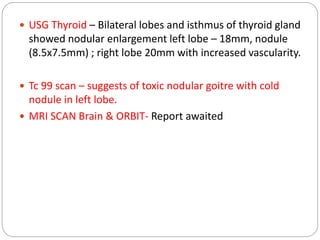
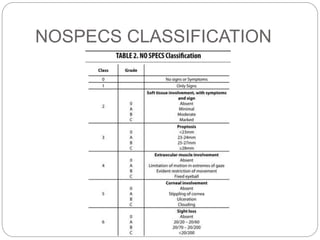
This document presents the case of a 55-year-old male with a 3-year history of a neck swelling and 2-year history of bulging eyes. On examination, he has a multinodular goiter and signs of thyroid eye disease. Investigations show biochemical hyperthyroidism and imaging confirms a toxic nodular goiter with orbit involvement. He is diagnosed with toxic nodular goiter grade II and thyroid eye disease stage 2B, 3A, 4A, 5, and 6A based on the NOSPECS classification system. He is being treated with anti-thyroid medications and lubricating eye drops with plans for regular follow up.