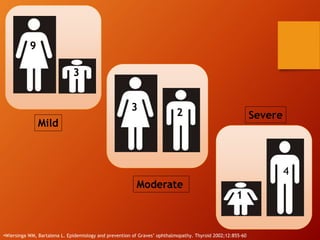
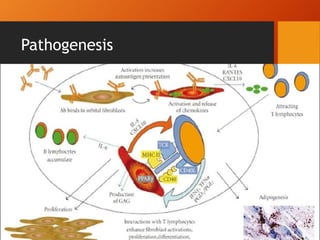
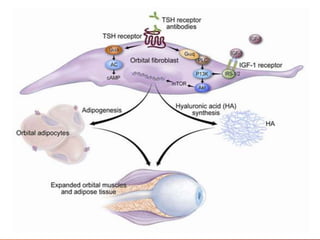
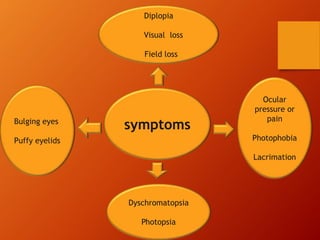
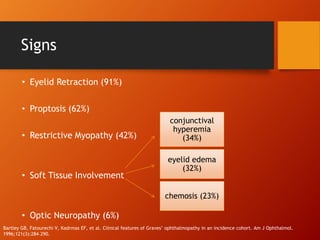
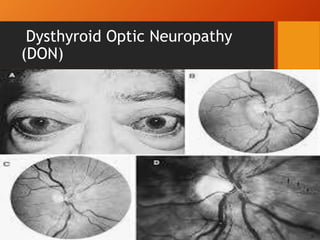
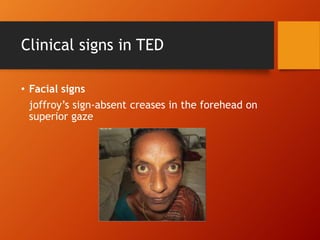
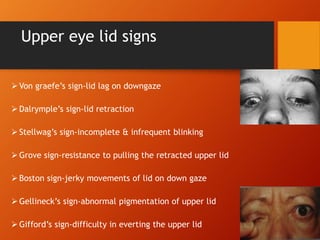
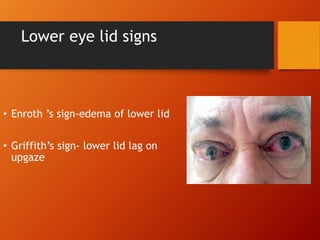
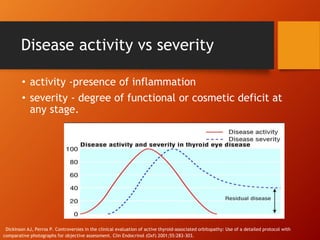
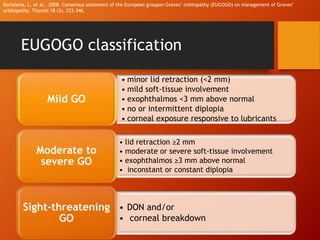
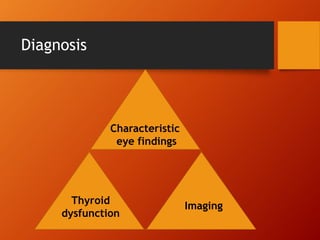
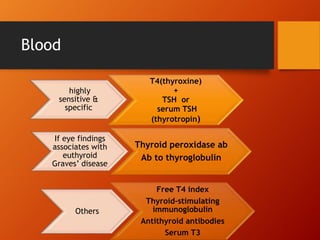
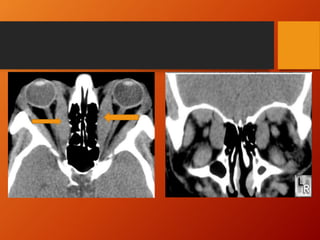
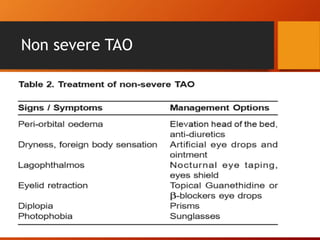
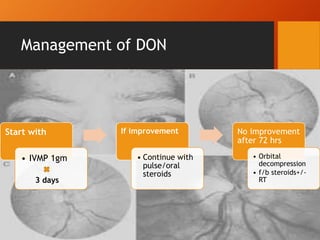
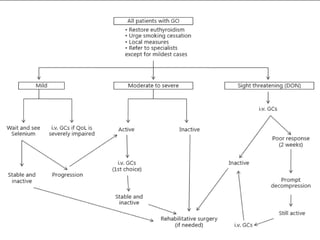
Thyroid eye disease, also known as Graves' ophthalmopathy, is an autoimmune condition causing inflammation and accumulation of fluid in the orbit, raising pressure. It produces symptoms related to proptosis, extraocular muscle involvement, and soft tissue changes. Management involves treatment of thyroid dysfunction, artificial tears, tobacco cessation, immunosuppression with steroids for moderate to severe disease, and orbital decompression or strabismus surgery for complications like dysthyroid optic neuropathy or diplopia. The disease progresses through inflammatory and fibrotic phases, and different classification systems evaluate severity and activity to guide treatment.