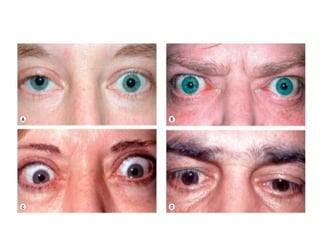
Thyroid eye disease is a manifestation of Graves' disease, an autoimmune disorder where antibodies stimulate excessive thyroid hormone production. The eyes may become inflamed, with soft tissue swelling leading to eyelid retraction, bulging eyes, and impaired eye movement. There are two stages: an initial inflammatory stage causing redness and pain, and a later fibrotic stage causing dry eyes and motility issues. Treatment focuses on reducing inflammation with lubricants, steroids, radiation or surgery to correct eye muscle fibrosis and positioning. Unchecked disease can cause vision loss due to optic nerve compression.