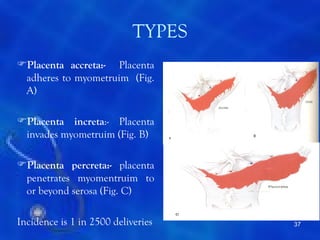
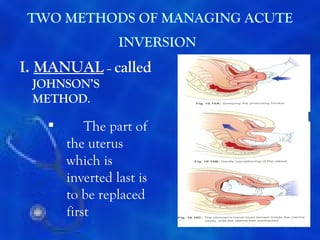
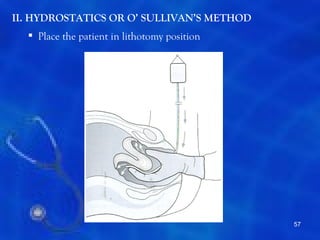
This document provides information on the management of the third stage of labour and complications. It discusses the three phases of the third stage, signs of placental separation, and mechanisms of controlling bleeding. It describes expectant and active management approaches. For retained placenta, steps include uterine massage, oxytocics, and controlled cord traction. Manual removal under anesthesia may be needed. Complications include postpartum hemorrhage, retained placenta, uterine inversion, and shock. Risk factors, diagnosis, and conservative management are outlined for morbidly adherent placenta such as placenta accreta.