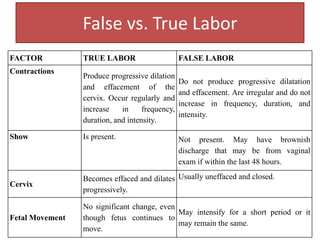
The document discusses the physiology of labor, including theories of labor initiation and premonitory signs that labor is imminent. It describes the stages of uterine contractions that characterize true labor, cervical changes like effacement and dilation, and other signs like bloody show. Nursing considerations are outlined for events like rupture of membranes, including actions to take for problems like cord prolapse.