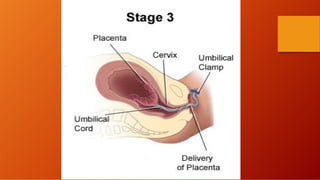
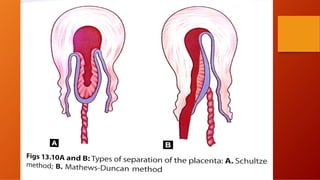
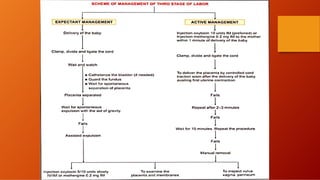
The third stage of labour involves the separation and expulsion of the placenta and membranes from the uterus. There are two main methods for managing the third stage - active management and expectant management. Active management involves providing oxytocin or methylergonovine within 1 minute of birth to help the uterus contract and quickly deliver the placenta, usually within 30 minutes. Expectant management allows the placenta to separate and deliver spontaneously on its own timeline, with close monitoring by a healthcare provider. After delivery of the placenta, the provider examines it and membranes for completeness and abnormalities before repairing any perineal trauma from birth.
























































![BMW[1].pptx community health nursing-2..](https://cdn.slidesharecdn.com/ss_thumbnails/bmw1-240521182705-3424b4e1-thumbnail.jpg?width=640&height=640&fit=bounds)
































