Downloaded 1,330 times



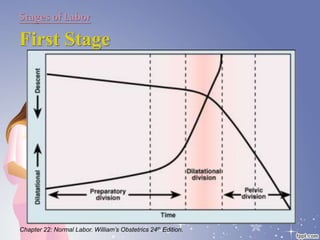
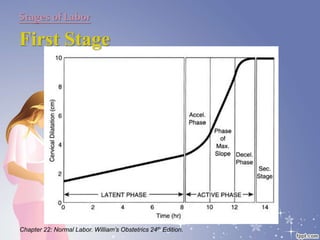
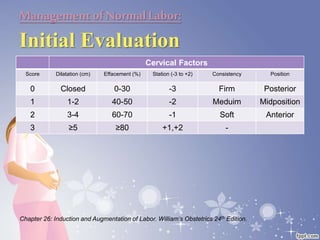
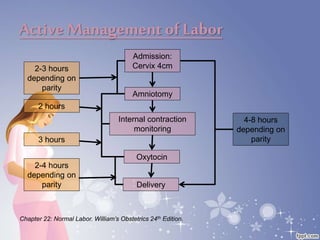


This document summarizes the normal labor and delivery process. It defines labor as beginning with regular uterine contractions and ending with childbirth. Labor involves three stages - first stage is cervical dilation from 0-10cm, second stage is birth of the baby, and third is delivery of the placenta. Key aspects of managing normal labor are admitting women in early labor, monitoring the fetus, allowing freedom of movement, and active management including amniotomy and oxytocin to shorten stages of labor. The goal is a safe birth for both mother and child with minimal medical intervention.



































































