

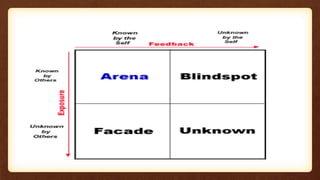
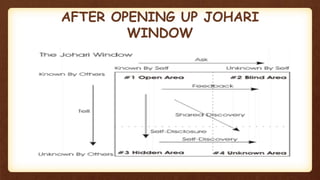


This document discusses therapeutic barriers and the Johari window model of communication. It defines attitudes and identifies various barriers to therapeutic communication, including physiological, social, cultural, ethical, psychological, language, physical, systematic, attitudinal and organizational barriers. The Johari window model has four quadrants representing the open self (known to self and others), private self (known to self but not others), unknown self (known to others but not self), and unknown self (unknown to self and others). Understanding these barriers and using the Johari window can help improve self-awareness, communication, relationships and group dynamics.













































































