Downloaded 1,977 times

![AECI/ARB COMBINED
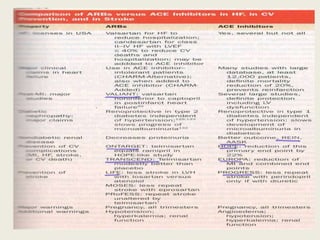
cardiovascular outcomes [ CHARM-Added, Val-HeFT, VALIANT vs
RESOLVD Pilot Study Investigators ] may relate to different
patient populations, previous or concurrent successful treatment
with other drugs, or study design
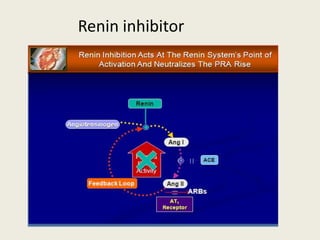
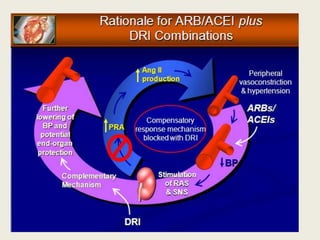
PRA is related to adverse clinical outcomes further raises the
possibility that DRIs may be useful.
In heart failure –FDA approved](https://image.slidesharecdn.com/therenin-angiotensinaldosteronesystem-final-120401080848-phpapp02/85/The-renin-angiotensin-aldosterone-system-51-320.jpg)

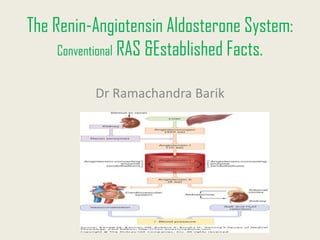
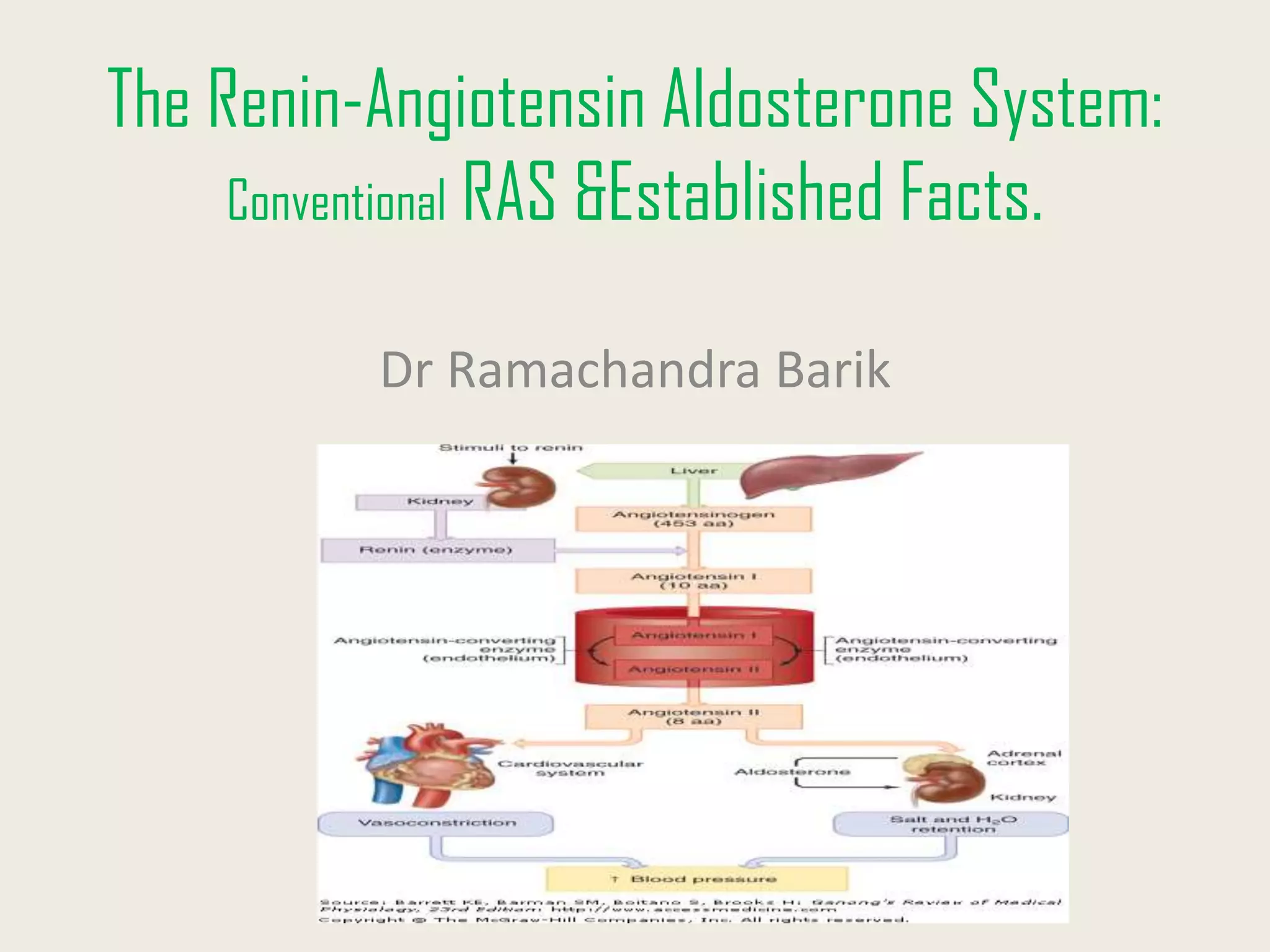
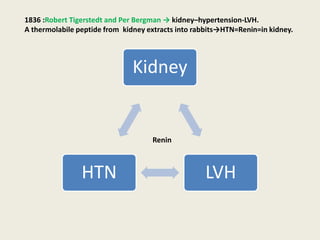
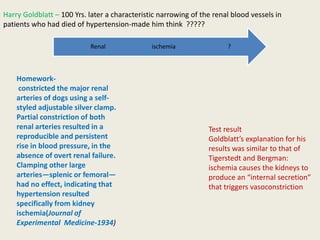
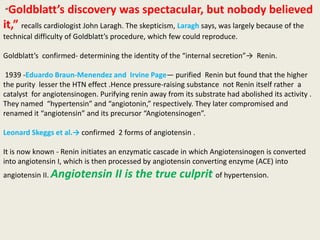
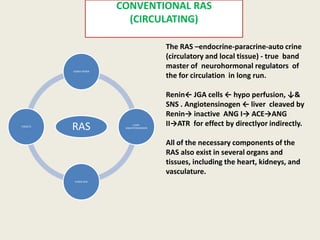
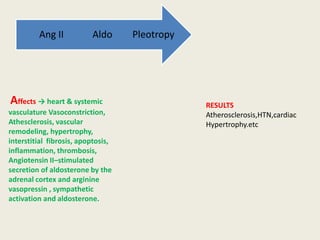
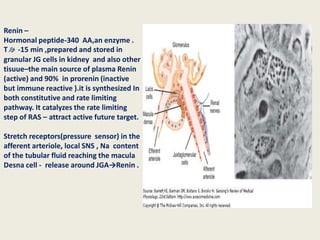
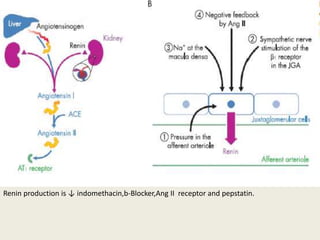
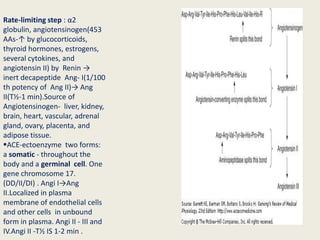
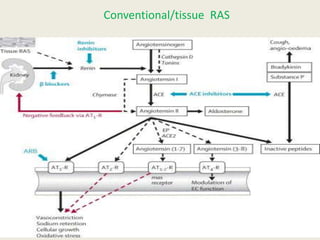
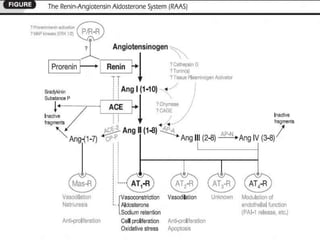
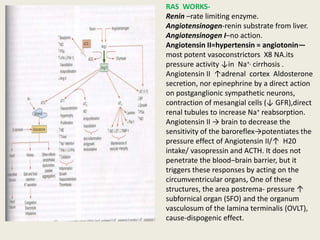
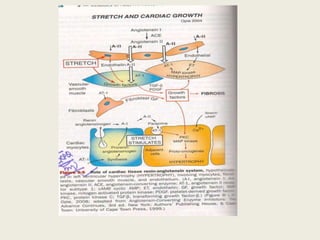
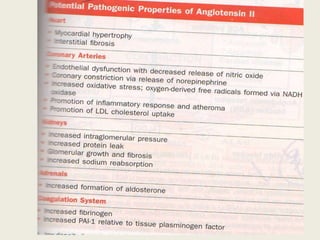
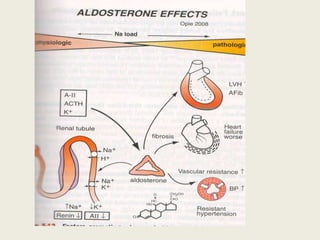
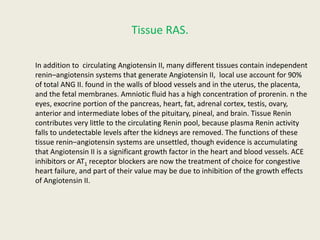
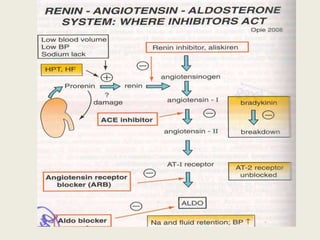
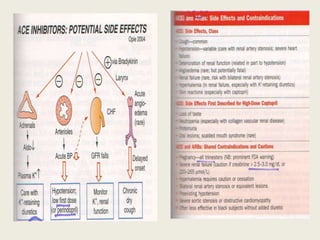
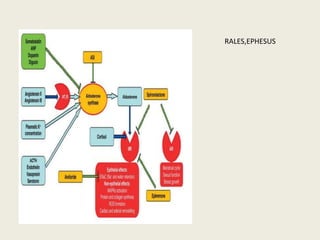
The Renin-Angiotensin Aldosterone System (RAAS) is the most potent vasoconstrictor system in the body. It was discovered in the 1930s-1940s through experiments involving renal artery clamping and purification of renin. The key components of the conventional circulating RAAS include renin from the kidneys, angiotensinogen from the liver, angiotensin I and II produced via enzymatic cascades, and aldosterone from the adrenal cortex. Angiotensin II is the primary effector peptide and causes vasoconstriction, hypertension, atherosclerosis, and other effects by activating AT1 receptors. Local tissue RAAS also exist and influence organ function.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















